

Cognition in chronic kidney disease: a systematic review and meta-analysis
- PMID: 27964726
- PMCID: PMC5155375
- DOI: 10.1186/s12916-016-0745-9
Cognition in chronic kidney disease: a systematic review and meta-analysis
Abstract
Background: Cognitive impairment is common in people with chronic kidney disease (CKD) and associated with increased morbidity and mortality. Subtle changes can impact engagement with healthcare, comprehension, decision-making, and medication adherence. We aimed to systematically summarise evidence of cognitive changes in CKD.
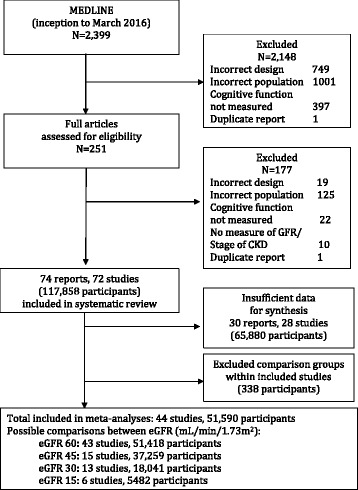
Methods: We searched MEDLINE (March 2016) for cross-sectional, cohort or randomised studies that measured cognitive function in people with CKD (PROSPERO, registration number CRD42014015226). The CKD population included people with eGFR < 60 mL/min/1.73 m2, not receiving renal replacement therapy, in any research setting. We conducted a meta-analysis using random effects, expressed as standardised mean differences (SMD) with 95% confidence intervals (CI). Outcomes were performance in eight cognitive domains. Bias was assessed with the Newcastle-Ottawa Scale (NOS).
Results: We identified 44 studies reporting sufficient data for synthesis (51,575 participants). Mean NOS score for cohort studies was 5.8/9 and for cross-sectional 5.4/10. Studies were deficient in NOS outcome and selection due to poor methods reporting and in comparison group validity of demographics and chronic disease status. CKD patients (eGFR < 60 mL/min/1.73 m2) performed worse than control groups (eGFR ≥ 60 mL/min/1.73 m2) on Orientation & Attention (SMD -0.79, 95% CI, -1.44 to -0.13), Language (SMD -0.63, 95% CI, -0.85 to -0.41), Concept Formation & Reasoning (SMD -0.63, 95% CI, -1.07 to -0.18), Executive Function (SMD -0.53, 95% CI, -0.85 to -0.21), Memory (SMD -0.48, 95% CI, -0.79 to -0.18), and Global Cognition (SMD -0.48, 95% CI, -0.72 to -0.24). Construction & Motor Praxis and Perception were unaffected (SMD -0.29, 95% CI, -0.90 to 0.32; SMD -1.12, 95% CI, -4.35 to 2.12). Language scores dropped with eGFR (<45 mL/min/1.73 m2 SMD -0.86, 95% CI, -1.25 to -46; 30 mL/min/1.73 m2 SMD -1.56, 95% CI, -2.27 to -0.84). Differences in Orientation & Attention were greatest at eGFR < 45 mL/min/1.73 m2 (SMD -4.62, 95% CI, -4.68 to -4.55). Concept Formation & Reasoning differences were greatest at eGFR < 45 mL/min/1.73 m2 (SMD -4.27, 95% CI, -4.23 to -4.27). Differences in Executive Functions were greatest at eGFR < 30 mL/min/1.73 m2 (SMD -0.54, 95% CI, -1.00 to -0.08).
Conclusions: Cognitive changes occur early in CKD, and skills decline at different rates. Orientation & Attention and Language are particularly affected. The cognitive impact of CKD is likely to diminish patients' capacity to engage with healthcare decisions. An individual's cognitive trajectory may deviate from average.
Keywords: Chronic kidney disease; Cognition; Dementia; Mild cognitive impairment; Neuropsychological tests; Psychometrics; Renal insufficiency.
Figures




References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
