

Mortality in children diagnosed with tuberculosis: a systematic review and meta-analysis
- PMID: 27964822
- PMCID: PMC5330933
- DOI: 10.1016/S1473-3099(16)30474-1
Mortality in children diagnosed with tuberculosis: a systematic review and meta-analysis
Abstract
Background: Case fatality ratios in children with tuberculosis are poorly understood-particularly those among children with HIV and children not receiving tuberculosis treatment. We did a systematic review of published work to identify studies of population-representative samples of paediatric (ie, <15 years) tuberculosis cases.
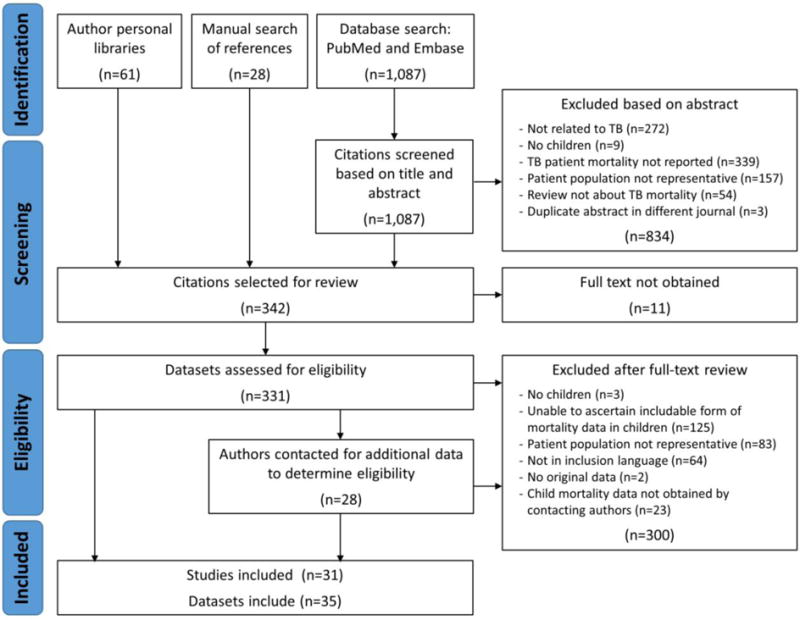
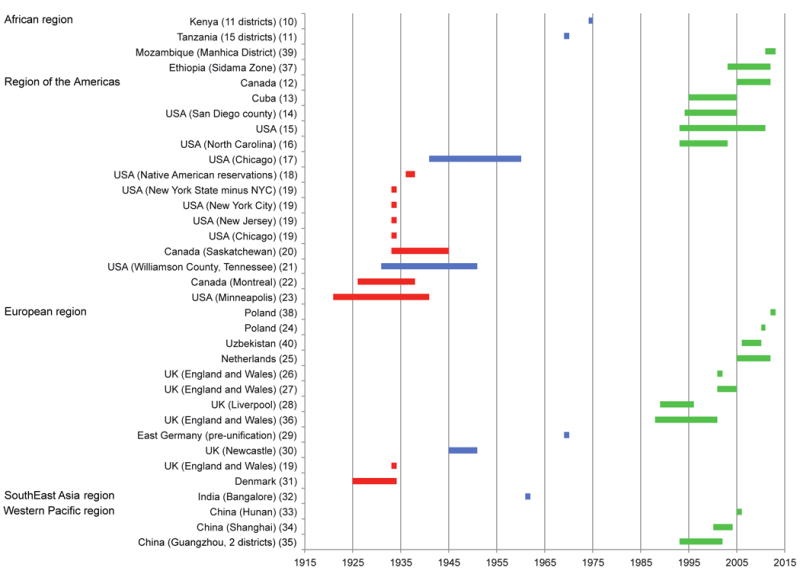
Methods: We searched PubMed and Embase for reports published in English, French, Portuguese, or Spanish before Aug 12, 2016, that included terms related to tuberculosis, children, mortality, and population representativeness. We also reviewed our own files and reference lists of articles identified by this search. We screened titles and abstracts for inclusion, excluding studies in which outcomes were unknown for 10% or more of the children and publications detailing non-representative samples. We used random-effects meta-analysis to produce pooled estimates of case fatality ratios from the included studies, which we divided into three eras: the pre-treatment era (ie, studies before 1946), the middle era (1946-80), and the recent era (after 1980). We stratified our analyses by whether or not children received tuberculosis treatment, age (0-4 years, 5-14 years), and HIV status.
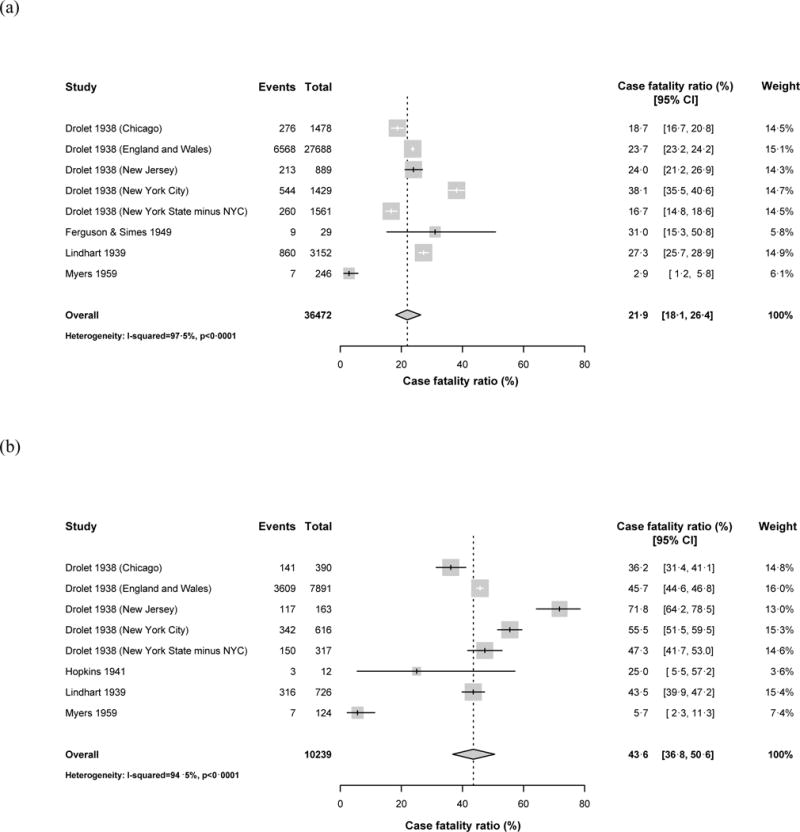
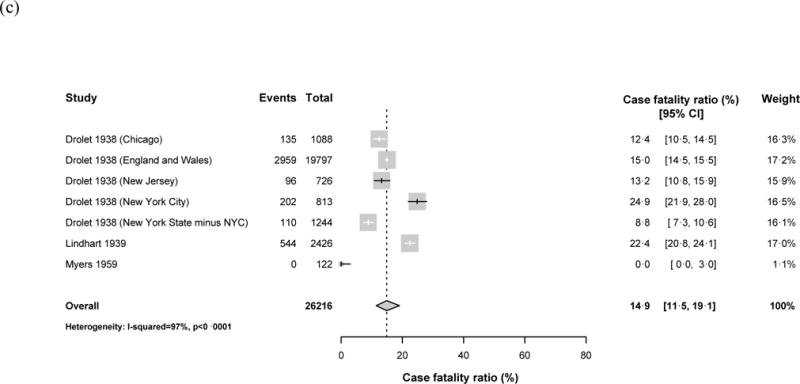
Findings: We identified 31 papers comprising 35 datasets representing 82 436 children with tuberculosis disease, of whom 9274 died. Among children with tuberculosis included in studies in the pre-treatment era, the pooled case fatality ratio was 21·9% (95% CI 18·1-26·4) overall. The pooled case fatality ratio was significantly higher in children aged 0-4 years (43·6%, 95% CI 36·8-50·6) than in those aged 5-14 years (14·9%, 11·5-19·1). In studies in the recent era, when most children had tuberculosis treatment, the pooled case fatality ratio was 0·9% (95% CI 0·5-1·6). US surveillance data suggest that the case fatality ratio is substantially higher in children with HIV receiving treatment for tuberculosis (especially without antiretroviral therapy) than in those without HIV.
Interpretation: Without adequate treatment, children with tuberculosis, especially those younger than 5 years, are at high risk of death. Children with HIV have an increased mortality risk, even when receiving tuberculosis treatment.
Funding: US National Institutes of Health, Janssen Global Public Health.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Conflict of interest statement
HEJ received funding from the U.S. National Institutes of Health (Award number: K01AI102944). MCB, CMY, and CAR received funding from Janssen Global Public Health.
Figures
Comment in
-
Mortality in childhood tuberculosis: has there been progress?Lancet Infect Dis. 2017 Mar;17(3):239-241. doi: 10.1016/S1473-3099(16)30537-0. Epub 2016 Dec 8. Lancet Infect Dis. 2017. PMID: 27964821 No abstract available.
References
-
- Dodd PJ, Gardiner E, Coghlan R, Seddon JA. Burden of childhood tuberculosis in 22 high-burden countries: a mathematical modelling study. The Lancet Global health. 2014;2(8):e453–9. - PubMed
-
- World Health Organization. Global Tuberculosis Report 2015. Geneva: 2015.
-
- Setel PW, Whiting DR, Hemed Y, et al. Validity of verbal autopsy procedures for determining cause of death in Tanzania. Trop Med Int Health. 2006;11(5):681–96. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
