

Rare cause of back pain: Staphylococcus aureus vertebral osteomyelitis complicated by recurrent epidural abscess and severe sepsis
- PMID: 27965310
- PMCID: PMC5174821
- DOI: 10.1136/bcr-2016-217111
Rare cause of back pain: Staphylococcus aureus vertebral osteomyelitis complicated by recurrent epidural abscess and severe sepsis
Abstract
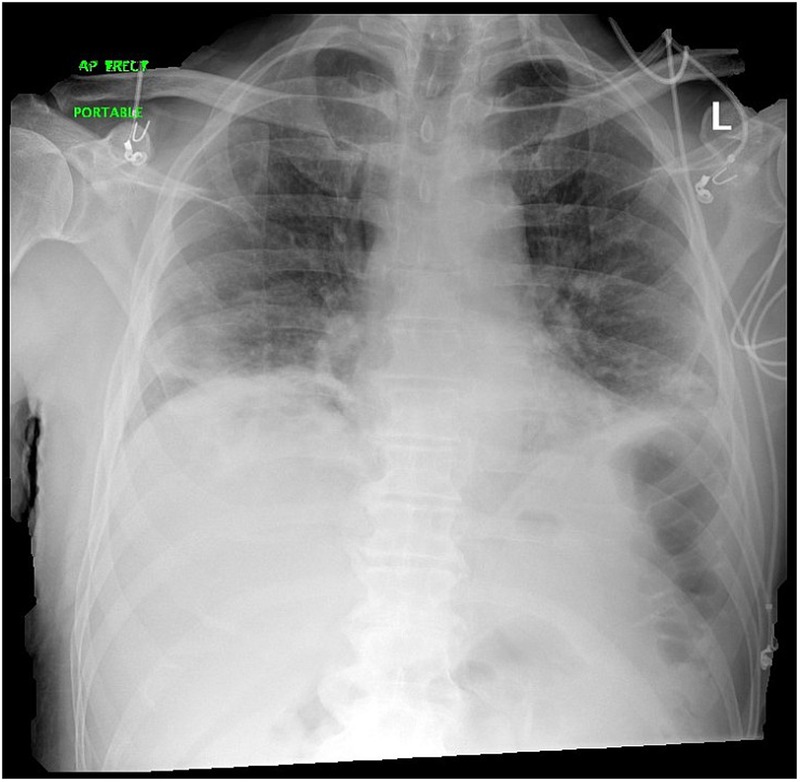
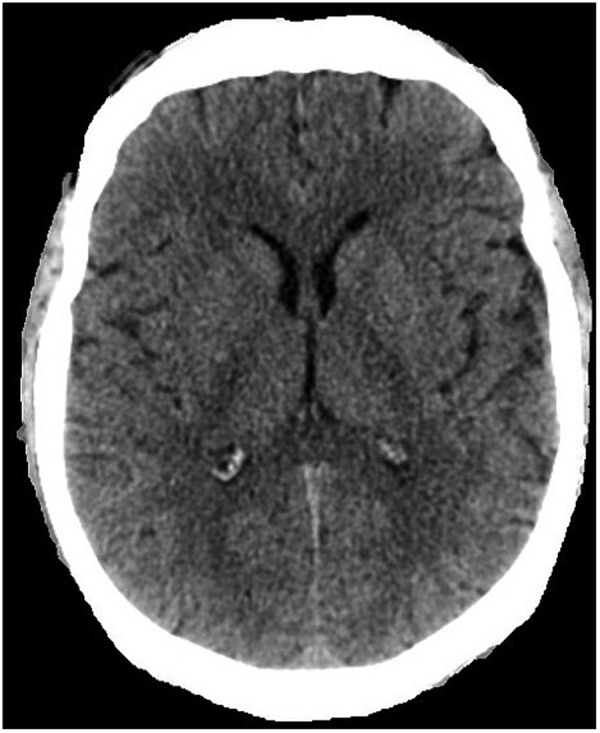
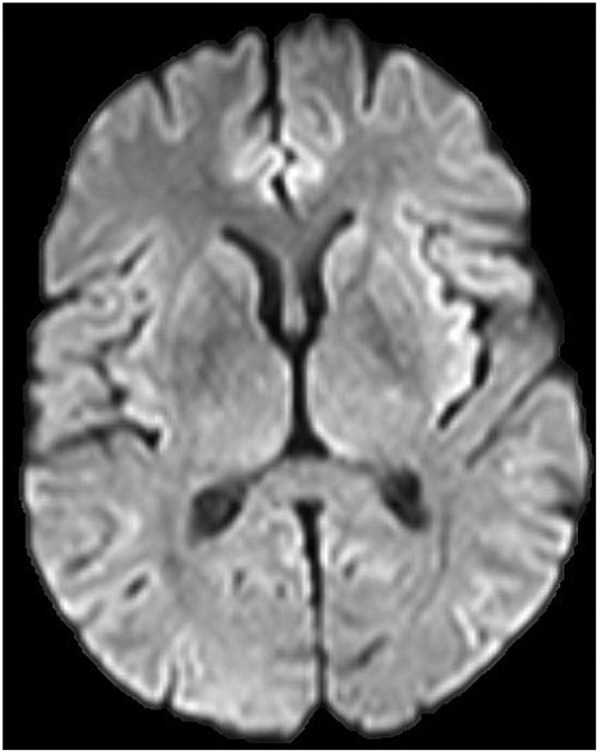
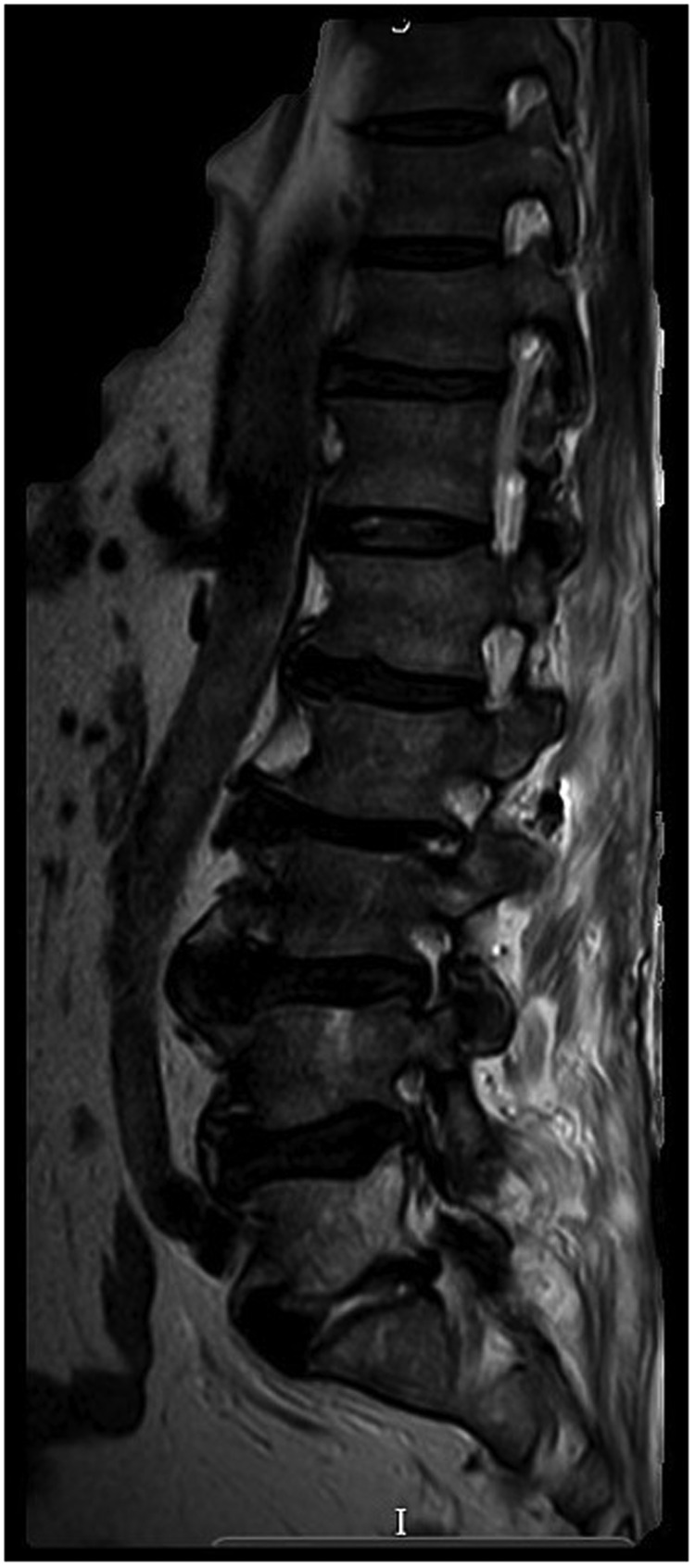
An epidural abscess represents a rare acute medical emergency, with a reported incidence of 2.5/10 000 hospital admissions annually. The clinical features include fever, spinal pain, radiating nerve root pain and leg weakness. When sepsis is present, prompt recognition is required to initiate appropriate antimicrobial therapy and surgical decompression. We present the case of a man aged 68 years presenting to the emergency department with a 3-day history of fever, low back, right hip and leg pain. He was hypoxic, tachycardic and hypotensive. He required intubation and ventilation. An MRI spine confirmed a posterior epidural abscess from T12 to L4. Blood cultures revealed Staphylococcus aureus He started treatment with linezolid and underwent incision and drainage. He remained septic and 8 days later, a repeat MRI spine showed a peripherally enhancing posterior epidural collection from L2/L3 to L4/L5, consistent with a recurrent epidural abscess. Further drainage was performed. He developed bilateral knee pain requiring washout. His right knee synovial biopsy cultured S. aureus He continued treatment with linezolid for 6 weeks until his C reactive protein was 0.8 ng/L. He started neurorehabilitation. 10 weeks later, he became feverish with lumbar spine tenderness. An MRI spine showed discitis of the L5/S1 endplate. A CT-guided biopsy confirmed discitis and osteomyelitis. Histology was positive for S. aureus and he started treatment with oral linezolid. After 19 days, he was discharged with 1 week of oral linezolid 600 mg 2 times per day, followed by 1 further week of oral clindamycin 600 mg 4 times daily. This case report reinforces the importance of maintaining a high clinical suspicion, with a prompt diagnosis and combined medical and surgical treatment to prevent adverse outcomes in this patient cohort. With spinal surgical services centralised, physicians may not encounter this clinical diagnosis more often in day-to-day hospital medical practice. The unique aspect of this case is the persistence and then the recurrence (despite 6 weeks of antimicrobial therapy and a second debridement) of S. aureus infection. Furthermore, the paucity of clinical recommendations and the controversy regarding the adequate duration of antimicrobial therapy are notable features of this case.
2016 BMJ Publishing Group Ltd.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures





Similar articles
-
Lumbosacral spondylodiscitis complicated by sepsis, osteomyelitis, epidural abscess formation and deep vein thrombosis.BMJ Case Rep. 2020 Dec 28;13(12):e238522. doi: 10.1136/bcr-2020-238522. BMJ Case Rep. 2020. PMID: 33372019 Free PMC article.
-
A Case of Methicillin-Sensitive Staphylococcus aureus (MSSA) Prostate Abscess, Osteomyelitis, and Myositis Associated with MSSA Bacteremia in a 60-Year-Old Patient Presenting with Back Pain.Am J Case Rep. 2022 Jul 2;23:e936704. doi: 10.12659/AJCR.936704. Am J Case Rep. 2022. PMID: 35778821 Free PMC article.
-
Spinal epidural abscess successfully treated with percutaneous, computed tomography-guided, needle aspiration and parenteral antibiotic therapy: case report and review of the literature.Neurosurgery. 2002 Aug;51(2):509-12; discussion 512. Neurosurgery. 2002. PMID: 12182793 Review.
-
Epidural abscess and discitis complicating instrumented posterior lumbar interbody fusion: a case report.Spine (Phila Pa 1976). 2004 Dec 1;29(23):E542-6. doi: 10.1097/01.brs.0000146802.38753.38. Spine (Phila Pa 1976). 2004. PMID: 15564903
-
A case report of iliopsoas abscess and literature review.Medicine (Baltimore). 2024 Aug 16;103(33):e39356. doi: 10.1097/MD.0000000000039356. Medicine (Baltimore). 2024. PMID: 39151535 Free PMC article. Review.
Cited by
-
Clinical Characteristics of Spinal Epidural Abscess Accompanied by Bacteremia.J Korean Neurosurg Soc. 2021 Jan;64(1):88-99. doi: 10.3340/jkns.2020.0278. Epub 2020 Dec 23. J Korean Neurosurg Soc. 2021. PMID: 33353288 Free PMC article.
-
Simultaneous occurrence of spinal epidural abscess and disk herniation causing irreversible neurologic deficits: A case report and review of the literature.Radiol Case Rep. 2018 Apr 25;13(3):719-723. doi: 10.1016/j.radcr.2018.03.020. eCollection 2018 Jun. Radiol Case Rep. 2018. PMID: 29721126 Free PMC article. No abstract available.
-
Spinal Infections: An Update.Microorganisms. 2020 Mar 27;8(4):476. doi: 10.3390/microorganisms8040476. Microorganisms. 2020. PMID: 32230730 Free PMC article. Review.
-
Surgical treatment of spondylodiscitis in critically ill septic patients.Acta Neurochir (Wien). 2023 Dec;165(12):3601-3612. doi: 10.1007/s00701-023-05748-7. Epub 2023 Aug 17. Acta Neurochir (Wien). 2023. PMID: 37587320 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous