

Frontline Science: HMGB1 induces neutrophil dysfunction in experimental sepsis and in patients who survive septic shock
- PMID: 27965385
- PMCID: PMC5433854
- DOI: 10.1189/jlb.5HI0316-128RR
Frontline Science: HMGB1 induces neutrophil dysfunction in experimental sepsis and in patients who survive septic shock
Abstract
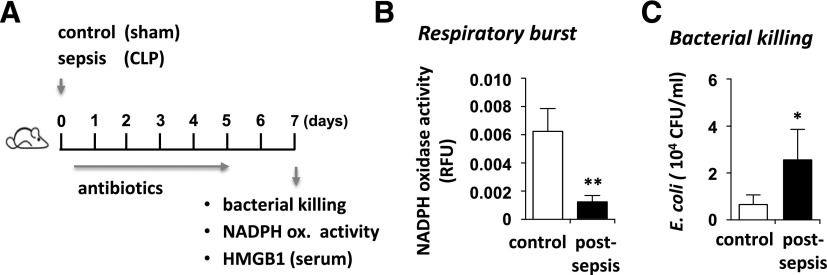
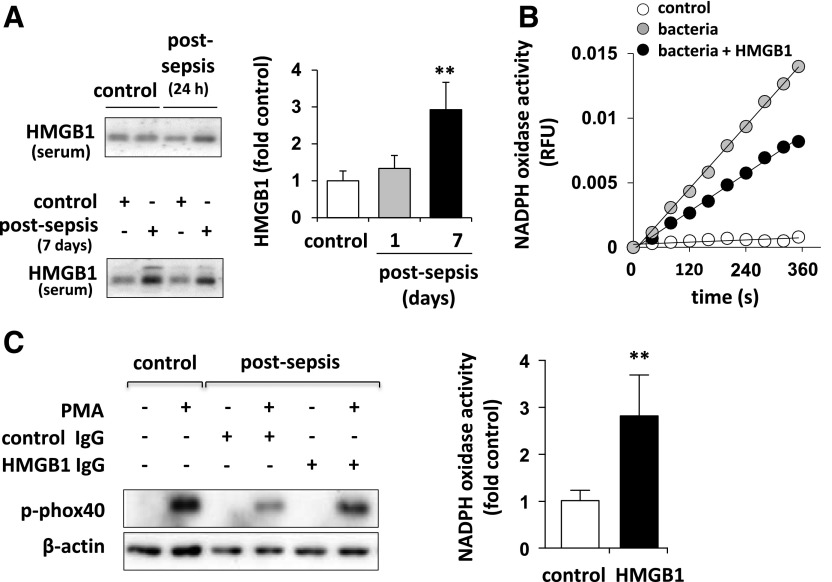
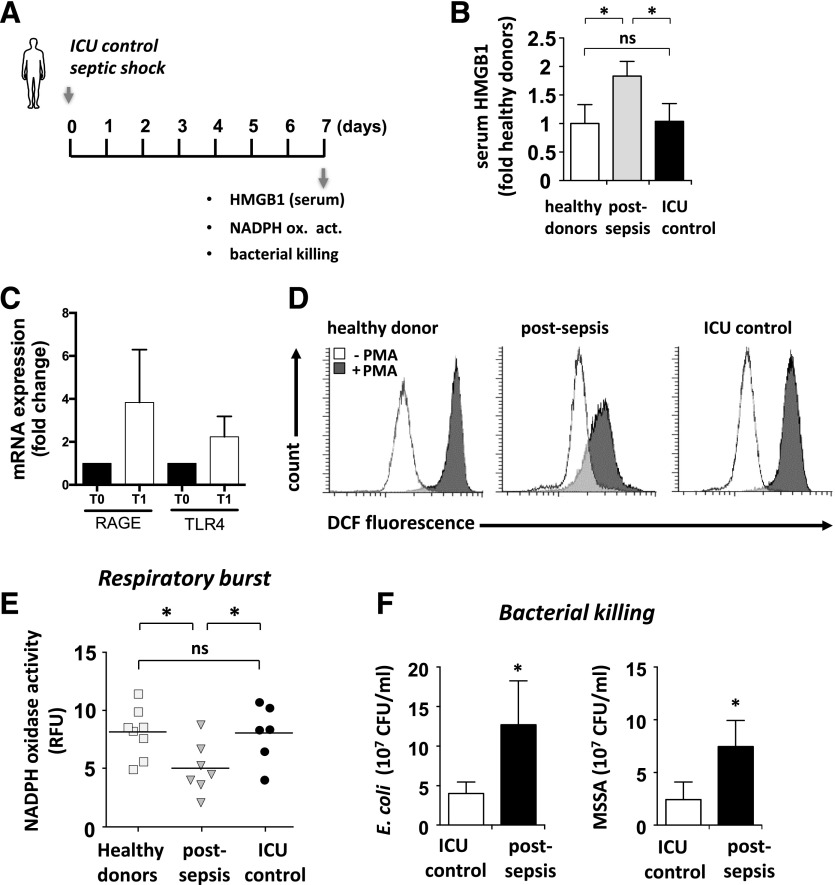
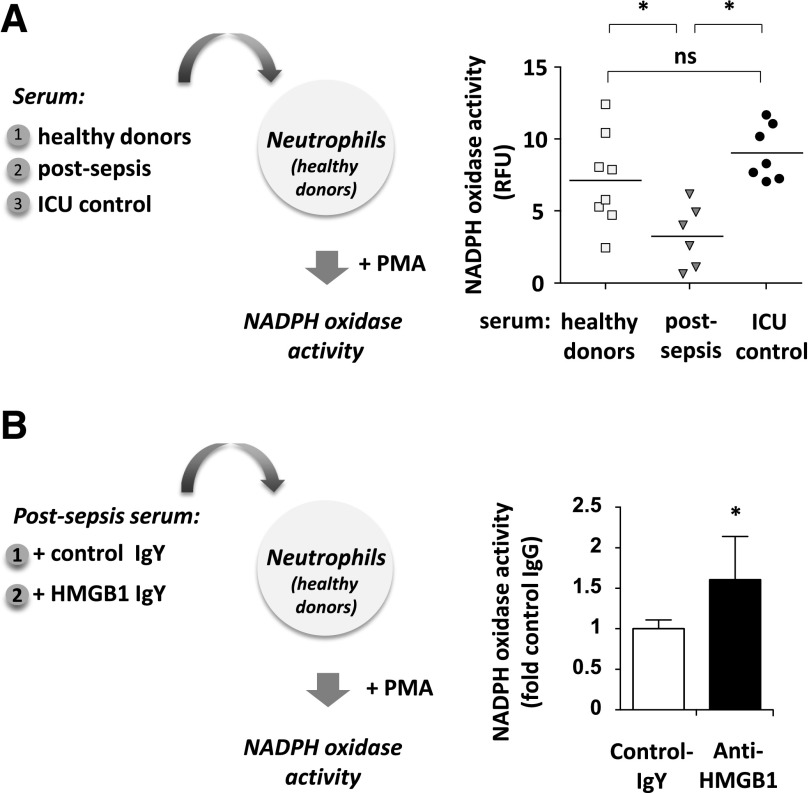
Sepsis is accompanied by the initial activation of proinflammatory pathways and long-lasting immunosuppression that appears to contribute to late-occurring mortality. Although high-mobility group box 1 (HMGB1) is involved in many aspects of inflammation, its role in sepsis-induced immune suppression remains unclear. In this study, we examined HMGB1's contribution to neutrophil NADPH oxidase activity dysfunction and associated neutrophil-dependent bacterial clearance in mice subjected to sepsis and in patients who survive septic shock. Using a murine model of polymicrobial septic peritonitis, we demonstrated that treatment with anti-HMGB1 Ab significantly diminished sepsis-induced dysfunction of neutrophil NADPH oxidase activity. In a subsequent set of experiments, we found that blocking HMGB1 preserved the ability of neutrophils from patients recovering from septic shock to activate NADPH oxidase. Taken together, our data suggest that HMGB1 accumulation in the late phase of sepsis plays a specific role in the development of postsepsis immunosuppression and specifically affects neutrophil-dependent antibacterial defense mechanisms. Thus, blocking HMGB1 may be a promising therapeutic intervention to diminish the adverse effects of sepsis-induced immunosuppression.
Keywords: HMGB1; NADPH oxidase; immunosuppression; neutrophils; sepsis.
© Society for Leukocyte Biology.
Figures
Comment in
-
Editorial: Modulation of HMGB1 holds promise for managing sepsis immune paralysis.J Leukoc Biol. 2017 Jun;101(6):1273-1275. doi: 10.1189/jlb.3CE1216-510R. J Leukoc Biol. 2017. PMID: 28572270 No abstract available.
Similar articles
-
Differential activation of RAGE by HMGB1 modulates neutrophil-associated NADPH oxidase activity and bacterial killing.Am J Physiol Cell Physiol. 2012 Jan 1;302(1):C249-56. doi: 10.1152/ajpcell.00302.2011. Epub 2011 Oct 19. Am J Physiol Cell Physiol. 2012. PMID: 22012330 Free PMC article.
-
HMGB1 promotes neutrophil PD-L1 expression through TLR2 and mediates T cell apoptosis leading to immunosuppression in sepsis.Int Immunopharmacol. 2024 May 30;133:112130. doi: 10.1016/j.intimp.2024.112130. Epub 2024 Apr 21. Int Immunopharmacol. 2024. PMID: 38648712
-
Hemorrhagic shock activates lung endothelial reduced nicotinamide adenine dinucleotide phosphate (NADPH) oxidase via neutrophil NADPH oxidase.Am J Respir Cell Mol Biol. 2011 Mar;44(3):333-40. doi: 10.1165/rcmb.2009-0408OC. Epub 2010 Apr 23. Am J Respir Cell Mol Biol. 2011. PMID: 20418360 Free PMC article.
-
The Regulatory Role of High-Mobility Group Protein 1 in Sepsis-Related Immunity.Front Immunol. 2021 Jan 22;11:601815. doi: 10.3389/fimmu.2020.601815. eCollection 2020. Front Immunol. 2021. PMID: 33552058 Free PMC article. Review.
-
[The role of neutrophils in the mechanisms of sepsis].Arkh Patol. 2024;86(6):82-91. doi: 10.17116/patol20248606182. Arkh Patol. 2024. PMID: 39686902 Review. Russian.
Cited by
-
Location is the key to function: HMGB1 in sepsis and trauma-induced inflammation.J Leukoc Biol. 2019 Jul;106(1):161-169. doi: 10.1002/JLB.3MIR1218-497R. Epub 2019 Apr 4. J Leukoc Biol. 2019. PMID: 30946496 Free PMC article. Review.
-
Beneficial effects of citrulline enteral administration on sepsis-induced T cell mitochondrial dysfunction.Proc Natl Acad Sci U S A. 2022 Feb 22;119(8):e2115139119. doi: 10.1073/pnas.2115139119. Proc Natl Acad Sci U S A. 2022. PMID: 35173051 Free PMC article.
-
Fatal Clostridium septicum gas gangrene complicating ECMO: case report and review of literature.Access Microbiol. 2024 Aug 5;6(8):000825.v3. doi: 10.1099/acmi.0.000825.v3. eCollection 2024. Access Microbiol. 2024. PMID: 39104453 Free PMC article.
-
Targeting HMGB1 for the treatment of sepsis and sepsis-induced organ injury.Acta Pharmacol Sin. 2022 Mar;43(3):520-528. doi: 10.1038/s41401-021-00676-7. Epub 2021 May 26. Acta Pharmacol Sin. 2022. PMID: 34040166 Free PMC article. Review.
-
The immune suppressive properties of damage associated molecular patterns in the setting of sterile traumatic injury.Front Immunol. 2023 Aug 15;14:1239683. doi: 10.3389/fimmu.2023.1239683. eCollection 2023. Front Immunol. 2023. PMID: 37662933 Free PMC article. Review.
References
-
- Angus D. C., van der Poll T. (2013) Severe sepsis and septic shock. N. Engl. J. Med. 369, 840–851. - PubMed
-
- Boomer J. S., To K., Chang K. C., Takasu O., Osborne D. F., Walton A. H., Bricker T. L., Jarman S. D. II, Kreisel D., Krupnick A. S., Srivastava A., Swanson P. E., Green J. M., Hotchkiss R. S. (2011) Immunosuppression in patients who die of sepsis and multiple organ failure. JAMA 306, 2594–2605. - PMC - PubMed
-
- Benjamim C. F., Hogaboam C. M., Kunkel S. L. (2004) The chronic consequences of severe sepsis. J. Leukoc. Biol. 75, 408–412. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
