

Genetic Obesity and the Risk of Atrial Fibrillation: Causal Estimates from Mendelian Randomization
- PMID: 27974350
- PMCID: PMC5322057
- DOI: 10.1161/CIRCULATIONAHA.116.024921
Genetic Obesity and the Risk of Atrial Fibrillation: Causal Estimates from Mendelian Randomization
Abstract
Background: Observational studies have identified an association between body mass index (BMI) and incident atrial fibrillation (AF). Inferring causality from observational studies, however, is subject to residual confounding, reverse causation, and bias. The primary objective of this study was to evaluate the causal association between BMI and AF by using genetic predictors of BMI.
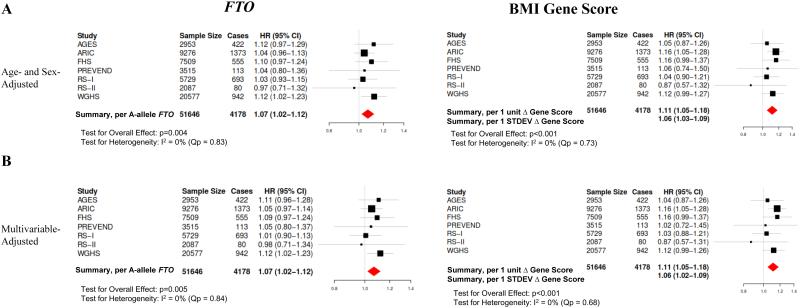
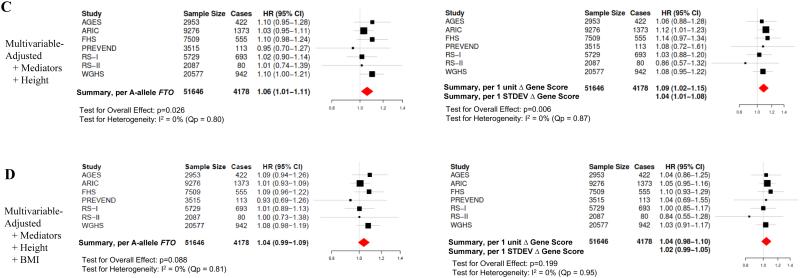
Methods: We identified 51 646 individuals of European ancestry without AF at baseline from 7 prospective population-based cohorts initiated between 1987 and 2002 in the United States, Iceland, and the Netherlands with incident AF ascertained between 1987 and 2012. Cohort-specific mean follow-up ranged from 7.4 to 19.2 years, over which period there was a total of 4178 cases of incident AF. We performed a Mendelian randomization with instrumental variable analysis to estimate a cohort-specific causal hazard ratio for the association between BMI and AF. Two genetic instruments for BMI were used: FTO genotype (rs1558902) and a BMI gene score comprising 39 single-nucleotide polymorphisms identified by genome-wide association studies to be associated with BMI. Cohort-specific estimates were combined by random-effects, inverse variance-weighted meta-analysis.
Results: In age- and sex-adjusted meta-analysis, both genetic instruments were significantly associated with BMI (FTO: 0.43 [95% confidence interval, 0.32-0.54] kg/m2 per A-allele, P<0.001; BMI gene score: 1.05 [95% confidence interval, 0.90-1.20] kg/m2 per 1-U increase, P<0.001) and incident AF (FTO, hazard ratio, 1.07 [1.02-1.11] per A-allele, P=0.004; BMI gene score, hazard ratio, 1.11 [1.05-1.18] per 1-U increase, P<0.001). Age- and sex-adjusted instrumental variable estimates for the causal association between BMI and incident AF were hazard ratio, 1.15 (1.04-1.26) per kg/m2, P=0.005 (FTO) and 1.11 (1.05-1.17) per kg/m2, P<0.001 (BMI gene score). Both of these estimates were consistent with the meta-analyzed estimate between observed BMI and AF (age- and sex-adjusted hazard ratio 1.05 [1.04-1.06] per kg/m2, P<0.001). Multivariable adjustment did not significantly change findings.
Conclusions: Our data are consistent with a causal relationship between BMI and incident AF. These data support the possibility that public health initiatives targeting primordial prevention of obesity may reduce the incidence of AF.
Keywords: atrial fibrillation; epidemiology; genetics; obesity; prevention & control.
© 2016 American Heart Association, Inc.
Figures

Comment in
-
Mendelian Randomization: Using Natural Genetic Variation to Assess the Causal Role of Modifiable Risk Factors in Observational Studies.Circulation. 2017 Feb 21;135(8):755-758. doi: 10.1161/CIRCULATIONAHA.117.026857. Circulation. 2017. PMID: 28223325 Free PMC article. No abstract available.
-
Letter by Koh Regarding Article, "Genetic Obesity and the Risk of Atrial Fibrillation: Causal Estimates from Mendelian Randomization".Circulation. 2017 Jul 25;136(4):432-433. doi: 10.1161/CIRCULATIONAHA.117.028130. Circulation. 2017. PMID: 28739817 No abstract available.
-
Response by Chatterjee et al to Letter Regarding Article, "Genetic Obesity and the Risk of Atrial Fibrillation: Causal Estimates From Mendelian Randomization".Circulation. 2017 Jul 25;136(4):434-435. doi: 10.1161/CIRCULATIONAHA.117.029035. Circulation. 2017. PMID: 28739818 Free PMC article. No abstract available.
References
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation. 2016;133(4):e38–e360. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22(8):983–988. - PubMed
-
- Wang TJ, Larson MG, Levy D, et al. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the Framingham Heart Study. Circulation. 2003;107(23):2920–2925. - PubMed
-
- Ott A, Breteler MM, de Bruyne MC, van Harskamp F, Grobbee DE, Hofman A. Atrial fibrillation and dementia in a population-based study. The Rotterdam Study. Stroke. 1997;28(2):316–321. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- N01 AG012100/AG/NIA NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- R01 HL128914/HL/NHLBI NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- R01 CA047988/CA/NCI NIH HHS/United States
- R01 HL080467/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- R01 HL087641/HL/NHLBI NIH HHS/United States
- K23 HL114724/HL/NHLBI NIH HHS/United States
- K24 HL105780/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201500001C/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- R01 HL092577/HL/NHLBI NIH HHS/United States
- R01 HL043851/HL/NHLBI NIH HHS/United States
- R01 HL059367/HL/NHLBI NIH HHS/United States
- 16EIA26410001/AHA/American Heart Association-American Stroke Association/United States
- T32 HL007575/HL/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- R01 HL086694/HL/NHLBI NIH HHS/United States
- U01 HG004402/HG/NHGRI NIH HHS/United States
- RC1 HL101056/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- R01 HL116690/HL/NHLBI NIH HHS/United States
- R01 HL102214/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- R21 HL093613/HL/NHLBI NIH HHS/United States
- HHSN268201500001I/HL/NHLBI NIH HHS/United States
- HHSN271201200022C/AG/NIA NIH HHS/United States
- UM1 CA182913/CA/NCI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- 2014105/DDCF/Doris Duke Charitable Foundation/United States
- RC1 HL099355/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
