

Regional Anaesthesia Is Associated with Shorter Postanaesthetic Care and Less Pain Than General Anaesthesia after Upper Extremity Surgery
- PMID: 27974889
- PMCID: PMC5128692
- DOI: 10.1155/2016/6308371
Regional Anaesthesia Is Associated with Shorter Postanaesthetic Care and Less Pain Than General Anaesthesia after Upper Extremity Surgery
Abstract
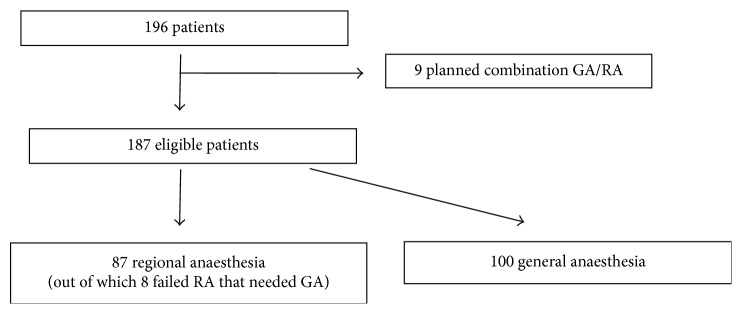
Introduction. For surgery on the upper extremity, the anaesthetist often has a choice between regional anaesthesia (RA) and general anaesthesia (GA). We sought to investigate the possible differences between RA and GA after upper extremity surgery with regard to postoperative patient comfort. Methods. This is a retrospective observational study that was performed at an acute care secondary referral centre. One hundred and eighty-seven procedures involving orthopaedic surgery on the upper extremity were included. The different groups (RA and GA) were compared regarding the primary outcome variable, length of stay in Postanaesthesia Unit, and secondary outcome variables, opioid consumption and nausea treatment. Results. RA was associated with significantly shorter median length of stay (99 versus 171 minutes). In the GA group, 32% of the patients received opioid analgesics and 21% received antiemetics. In the RA group, none received opioid analgesics and 3% received antiemetics. Conclusion. In this observational study, RA was superior to GA for surgery of the upper extremity regarding Postanaesthesia Care Unit length of stay, number of doses of analgesic, and number of doses of antiemetic administered.
Conflict of interest statement
None of the authors have any conflict of interests in relation to this manuscript.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
