

Reasons for the persistent incidence of venous thromboembolism
- PMID: 27975103
- PMCID: PMC5597250
- DOI: 10.1160/TH16-07-0509
Reasons for the persistent incidence of venous thromboembolism
Erratum in
-
Erratum to Heit et al. "Reasons for the persistent incidence of venous thromboembolism" (Thromb Haemost 2017; 117: 390-400).Thromb Haemost. 2017 Feb 28;117(3):643. doi: 10.1160/TH1703002. Thromb Haemost. 2017. PMID: 28245032 No abstract available.
Abstract
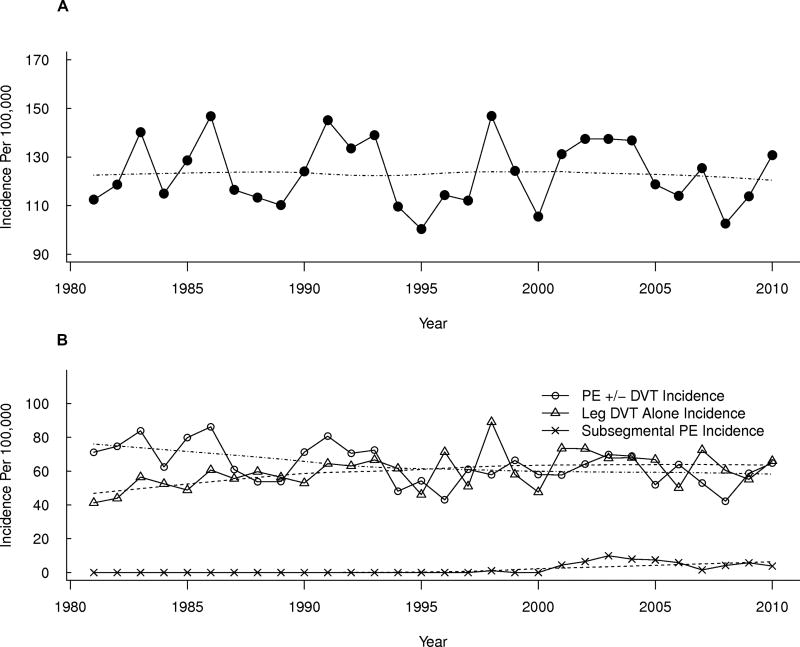
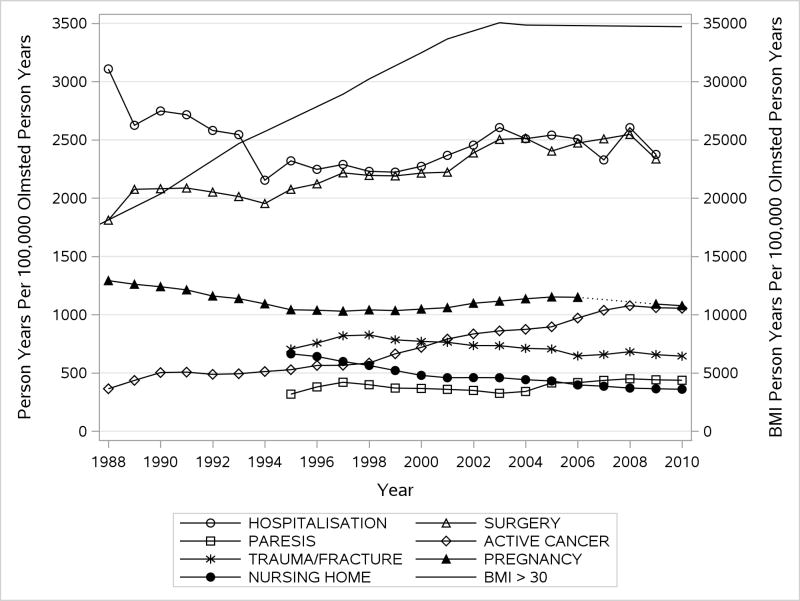
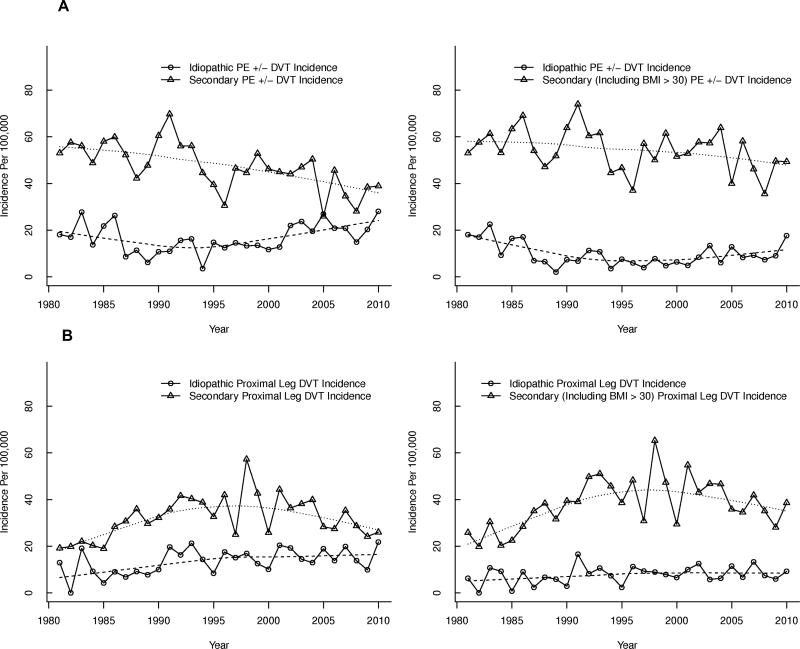
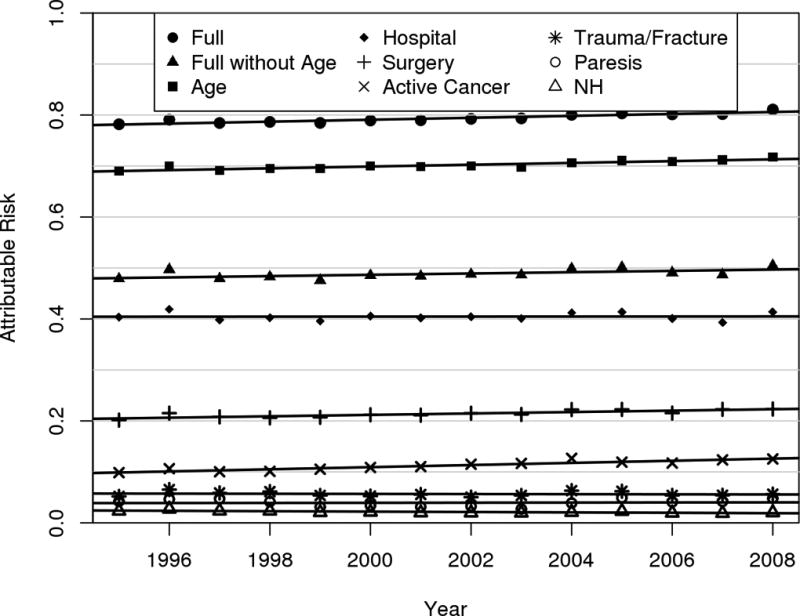
Reasons for trends in venous thromboembolism (VTE) incidence are uncertain. It was our objective to determine VTE incidence trends and risk factor prevalence, and estimate population-attributable risk (PAR) trends for each risk factor. In a population-based cohort study of all residents of Olmsted County, Minnesota from 1981-2010, annual incidence rates were calculated using incident VTE cases as the numerator and age- and sex-specific Olmsted County population estimates as the denominator. Poisson regression models were used to assess the relationship of crude incidence rates to year of diagnosis, age at diagnosis, and sex. Trends in annual prevalence of major VTE risk factors were estimated using linear regression. Poisson regression with time-dependent risk factors (person-years approach) was used to model the entire population of Olmsted County and derive the PAR. The age- and sex-adjusted annual VTE incidence, 1981-2010, did not change significantly. Over the time period, 1988-2010, the prevalence of obesity, surgery, active cancer and leg paresis increased. Patient age, hospitalisation, surgery, cancer, trauma, leg paresis and nursing home confinement jointly accounted for 79 % of incident VTE; obesity accounted for 33 % of incident idiopathic VTE. The increasing prevalence of obesity, cancer and surgery accounted in part for the persistent VTE incidence. The PAR of active cancer and surgery, 1981-2010, significantly increased. In conclusion, almost 80 % of incident VTE events are attributable to known major VTE risk factors and one-third of incident idiopathic VTE events are attributable to obesity. Increasing surgery PAR suggests that concurrent efforts to prevent VTE may have been insufficient.
Keywords: Venous thrombosis; epidemiology; phlebitis; pulmonary embolism; thrombophlebitis.
Conflict of interest statement
Dr. Heit declares no conflict of interest.
Dr. Ashrani declares no conflict of interest.
Mr. Crusan declares no conflict of interest.
Ms. Petterson declares no conflict of interest.
Dr. Bailey declares no conflict of interest.
Figures
References
-
- The Surgeon General’s Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism. U.S. Public Health Service 2008. U.S. Department of Health and Human Services. 2008
-
- Shojania K, Duncan B, McDonald K-SU, Wachter R. Making Health Care Safer: A Critical Analysis of Patient Safety Practices: UCSF-Stanford Evidence-Based Practice Center. Agency for Healthcare Research and Quality. 2001 Jul 20; Publication no. 01-E058, Evidence report no. 43. www.ahrq.gov/clinic/ptsafety/summary/htm; 2001. - PMC - PubMed
-
- Kahn SR, Lim W, Dunn AS, Cushman M, Dentali F, Akl EA, Cook DJ, Balekian AA, Klein RC, Le H, Schulman S, Murad MH. Prevention of VTE in nonsurgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141:e195S–226S. - PMC - PubMed
-
- Gould MK, Garcia DA, Wren SM, Karanicolas PJ, Arcelus JI, Heit JA, Samama CM. Prevention of VTE in nonorthopedic surgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141:e227S–277S. - PMC - PubMed
-
- Falck-Ytter Y, Francis CW, Johanson NA, Curley C, Dahl OE, Schulman S, Ortel TL, Pauker SG, Colwell CW., Jr Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141:e278S–325S. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
