

Sources of inaccuracy in the measurement of adult patients' resting blood pressure in clinical settings: a systematic review
- PMID: 27977471
- PMCID: PMC5278896
- DOI: 10.1097/HJH.0000000000001197
Sources of inaccuracy in the measurement of adult patients' resting blood pressure in clinical settings: a systematic review
Abstract
Background: To interpret blood pressure (BP) data appropriately, healthcare providers need to be knowledgeable of the factors that can potentially impact the accuracy of BP measurement and contribute to variability between measurements.
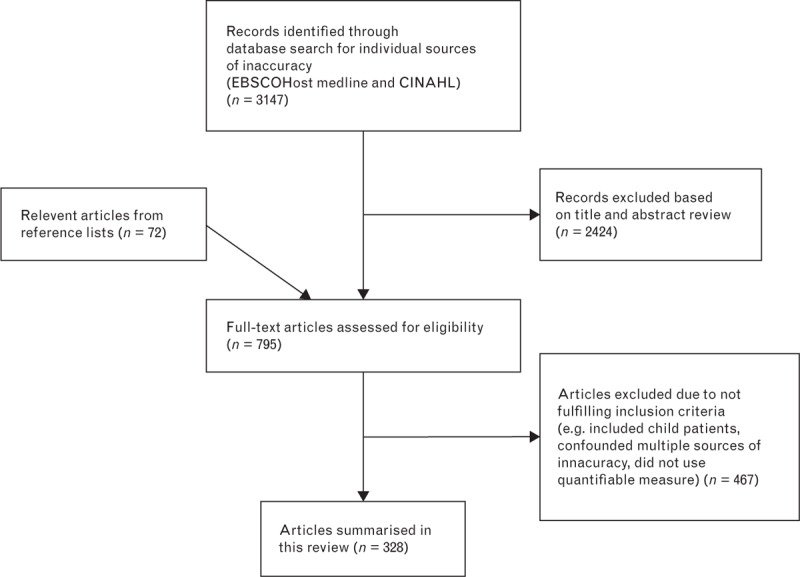
Methods: A systematic review of studies quantifying BP measurement inaccuracy. Medline and CINAHL databases were searched for empirical articles and systematic reviews published up to June 2015. Empirical articles were included if they reported a study that was relevant to the measurement of adult patients' resting BP at the upper arm in a clinical setting (e.g. ward or office); identified a specific source of inaccuracy; and quantified its effect. Reference lists and reviews were searched for additional articles.
Results: A total of 328 empirical studies were included. They investigated 29 potential sources of inaccuracy, categorized as relating to the patient, device, procedure or observer. Significant directional effects were found for 27; however, for some, the effects were inconsistent in direction. Compared with true resting BP, significant effects of individual sources ranged from -23.6 to +33 mmHg SBP and -14 to +23 mmHg DBP.
Conclusion: A single BP value outside the expected range should be interpreted with caution and not taken as a definitive indicator of clinical deterioration. Where a measurement is abnormally high or low, further measurements should be taken and averaged. Wherever possible, BP values should be recorded graphically within ranges. This may reduce the impact of sources of inaccuracy and reduce the scope for misinterpretations based on small, likely erroneous or misleading, changes.
Figures
References
-
- Jones D, Drennan K, Hart GK, Bellomo R, Web SAR. ANZICS-CORE MET Dose Investigators. Rapid Response Team composition, resourcing and calling criteria in Australia. Resuscitation 2012; 83:563–567. - PubMed
-
- Hollenberg S, Ahrens T, Annane D, Astiz M, Chalfin D, Dasta J, et al. Practice parameters for hemodynamic support of sepsis in adult patients: 2004 update. Crit Care Med 2004; 32:1928–1948. - PubMed
-
- Holley A, Lukin W, Paratz J, Hawkins T, Boots R, Lipman J. Review article: Part one: Goal-directed resuscitation – which goals? Haemodynamic targets. Emerg Med Australas 2012; 24:14–22. - PubMed
-
- Pickering TG, Hall JE, Appel LJ, Falkner BE, Graves J, Hill MN, et al. Recommendations for blood pressure measurement in humans and experimental animals: Part 1: Blood pressure measurement in humans: a statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Hypertension 2005; 45:142–161. - PubMed
-
- Williams B, Poulter NR, Brown MJ, Davis M, McInnes GT, Potter JF, et al. Guidelines for management of hypertension: report of the fourth working party of the British Hypertension Society, 2004 – BHS IV. J Human Hypertens 2004; 18:139–185. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
