

Diagnostic performance of convex probe EBUS-TBNA in patients with mediastinal and coexistent endobronchial or peripheral lesions
- PMID: 27977603
- PMCID: PMC5268049
- DOI: 10.1097/MD.0000000000005619
Diagnostic performance of convex probe EBUS-TBNA in patients with mediastinal and coexistent endobronchial or peripheral lesions
Abstract
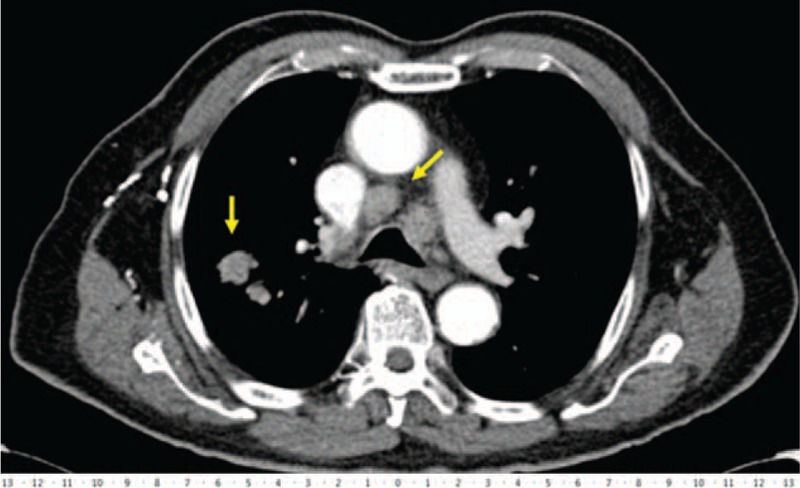
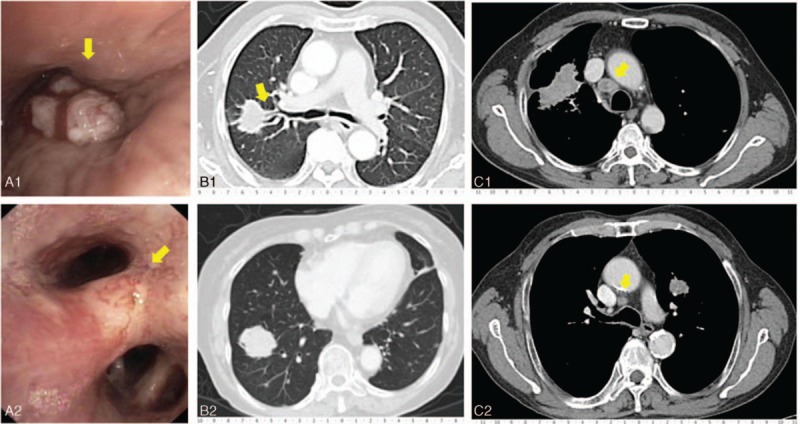
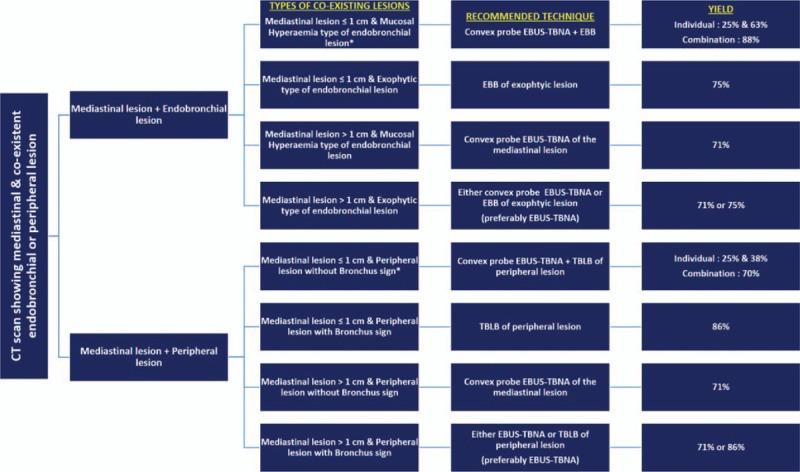
To compare the performance of convex probe endobronchial ultrasound guided transbronchial needle aspiration (EBUS-TBNA) with conventional endobronchial biopsy (EBB) or transbronchial lung biopsy (TBLB) in patients with mediastinal, and coexisting endobronchial or peripheral lesions.Retrospective review of records of patients undergoing diagnostic EBUS-TBNA and conventional bronchoscopy in 2014.A total of 74 patients had mediastinal, and coexisting endobronchial or peripheral lesions. The detection rate of EBUS-TBNA for mediastinal lesion >1 cm in short axis, EBB for visible exophytic type of endobronchial lesion, and TBLB for peripheral lesion with bronchus sign were 71%, 75%, and 86%, respectively. In contrast, the detection rate of EBUS-TBNA for mediastinal lesion ≤1 cm in short axis, EBB for mucosal hyperemia type of endobronchial lesion, and TBLB for peripheral lesion without bronchus sign were 25%, 63%, and 38%, and improved to 63%, 88%, and 62% respectively by adding EBB or TBLB to EBUS-TBNA, and EBUS-TBNA to EBB or TBLB. Postprocedure bleeding was significantly more common in patients undergoing EBB and TBLB 8 (40%) versus convex probe EBUS-TBNA 2 patients (2.7%, P = 0.0004).EBUS-TBNA is a safer single diagnostic technique compared with EBB or TBLB in patients with mediastinal lesion of >1 cm in size, and coexisting exophytic type of endobronchial lesion, or peripheral lesion with bronchus sign. However, it requires combining with EBB or TBLB and vice versa to optimize yield when mediastinal lesion is ≤1 cm in size, and coexisting endobronchial and peripheral lesions lack exophytic nature, and bronchus sign, respectively.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

Similar articles
-
Endobronchial ultrasound-guided transbronchial needle aspiration vs conventional transbronchial needle aspiration in the diagnosis of sarcoidosis.Chest. 2014 Sep;146(3):547-556. doi: 10.1378/chest.13-2339. Chest. 2014. PMID: 24481031 Clinical Trial.
-
Value of different bronchoscopic sampling techniques in diagnosis of sarcoidosis: a prospective study of 151 patients.J Bronchology Interv Pulmonol. 2014 Jul;21(3):220-6. doi: 10.1097/LBR.0000000000000081. J Bronchology Interv Pulmonol. 2014. PMID: 24992130
-
The role of EBUS-TBNA and standard bronchoscopic modalities in the diagnosis of sarcoidosis.Clin Respir J. 2017 Jan;11(1):58-63. doi: 10.1111/crj.12304. Epub 2015 May 26. Clin Respir J. 2017. PMID: 25919969
-
Endobronchial Ultrasound-Guided Transbronchial Mediastinal Cryobiopsy versus Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration for Mediastinal Disorders: A Meta-Analysis.Respiration. 2024;103(7):359-367. doi: 10.1159/000538609. Epub 2024 Apr 8. Respiration. 2024. PMID: 38588649
-
Advantages and drawbacks associated with the use of endosonography in sarcoidosis.Expert Rev Respir Med. 2023 Apr;17(4):267-277. doi: 10.1080/17476348.2023.2201439. Epub 2023 Apr 10. Expert Rev Respir Med. 2023. PMID: 37026845 Review.
Cited by
-
Video-Assisted Thoracic Surgery Core Needle Biopsy for Pulmonary Nodules in Patients with Impaired Lung Function: Is It Feasible and Safe?J Chest Surg. 2023 Jan 5;56(1):1-5. doi: 10.5090/jcs.22.063. J Chest Surg. 2023. PMID: 36598118 Free PMC article.
References
-
- Singh SP. The positive bronchus sign. Radiology 1998;209:251–2. - PubMed
-
- Naidich DP, Sussman R, Kutcher WL, et al. Solitary pulmonary nodules. CT-Bronchoscopic correlation. Chest 1988;93:595–8. - PubMed
-
- Gaeta M, Barone M, Russi EG, et al. Carcinomatous solitary pulmonary nodule: evaluation of tumor bronchi relationship with thin-section CT. Radiology 1993;187:535–9. - PubMed
-
- Bilaceroglu S, Kumcuoglu Z, Alper H, et al. CT-bronchus sign guided bronchoscopic multiple diagnostic procedures in carcinomatous pulmonary nodules and masses. Respiration 1998;65:49–55. - PubMed
-
- Gaeta M, Pandolfo I, Volta S, et al. Bronchus sign on CT in peripheral carcinoma of the lung. Value in predicting results of transbronchial biopsy. Am J Roengenol 1991;157:1181–5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
