

BRCAness as a Biomarker for Predicting Prognosis and Response to Anthracycline-Based Adjuvant Chemotherapy for Patients with Triple-Negative Breast Cancer
- PMID: 27977696
- PMCID: PMC5158199
- DOI: 10.1371/journal.pone.0167016
BRCAness as a Biomarker for Predicting Prognosis and Response to Anthracycline-Based Adjuvant Chemotherapy for Patients with Triple-Negative Breast Cancer
Abstract
Background: Triple-negative breast cancer (TNBC) is a heterogeneous tumor that encompasses many different subclasses of the disease. In this study, we assessed BRCAness, defined as the shared characteristics between sporadic and BRCA1-mutated tumors, in a large cohort of TNBC cases.
Methods: The BRCAness of 262 patients with primary TNBCs resected between January 2004 and December 2014 was determined through the isolation of DNA from tumor tissue. Classification of BRCAness was performed using multiple ligation-dependent probe amplification (MLPA). The tumor subtypes were determined immunohistochemically using resected specimens.
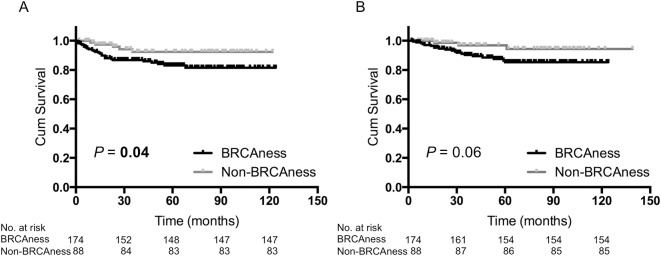
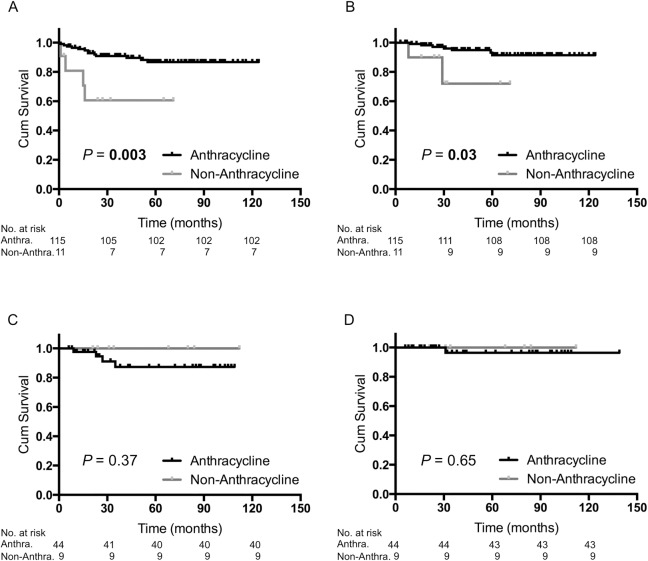
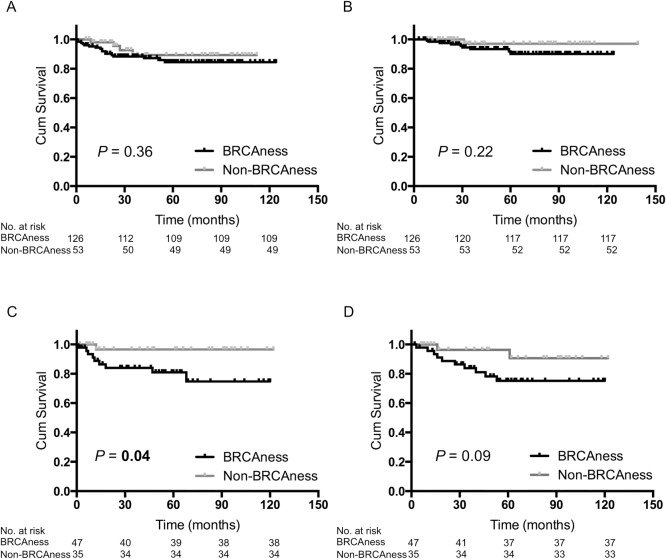
Results: Of the 262 TNBCs, the results of the MLPA assays showed that 174 (66.4%) tumors had BRCAness. Patients with BRCAness tumors were younger than patients with non-BRCAness tumors (P = 0.003). There was no significant difference between the two groups regarding their pathological stages. The BRCAness group had a significantly shorter recurrence-free survival (RFS) compared with the non-BRCAness group (P = 0.04) and had a shorter overall survival (OS) although this did not reach statistical significance. Adjuvant treatments with anthracycline-based regimens provided significantly greater benefits to the BRCAness group (P = 0.003 for RFS, and P = 0.03 for OS). Multivariate Cox proportional hazard model analysis showed that BRCAness was an independent negative prognostic factor, and the anthracycline-based adjuvant chemotherapy was an independent positive prognostic factor for both RFS and OS in TNBC.
Conclusions: The 66.4% patients of TNBCs showed BRCAness. BRCAness is essential as a biomarker in the subclassification of TNBCs and might be of use for predicting their prognosis. Furthermore, this biomarker might be a predictive factor for the effectiveness of anthracycline-based adjuvant chemotherapy for patients with TNBCs.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Dent R, Trudeau M, Pritchard KI, Hanna WM, Kahn HK, Sawka CA, et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res. 2007;13(15 Pt 1):4429–4434. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
