

Vitreoretinal instruments: vitrectomy cutters, endoillumination and wide-angle viewing systems
- PMID: 27980854
- PMCID: PMC5137208
- DOI: 10.1186/s40942-016-0052-9
Vitreoretinal instruments: vitrectomy cutters, endoillumination and wide-angle viewing systems
Abstract
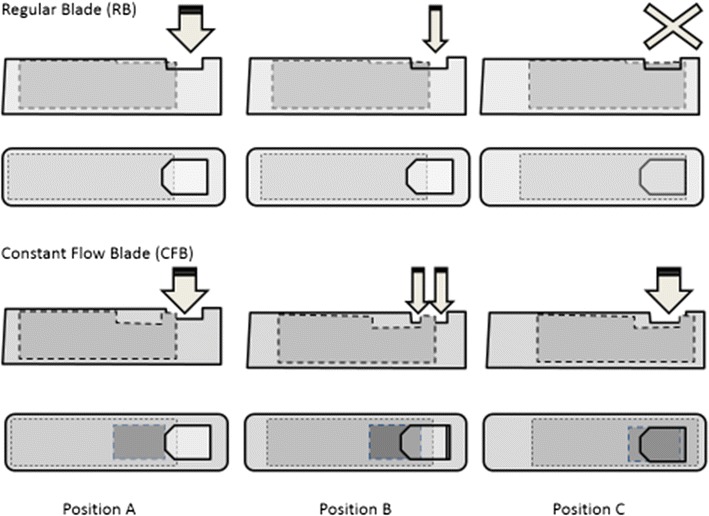
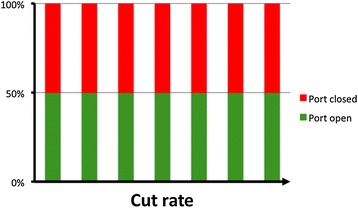
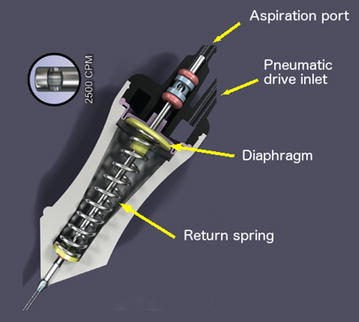
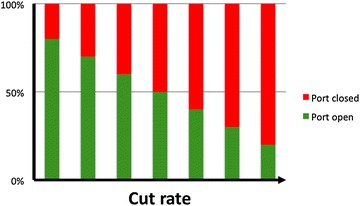
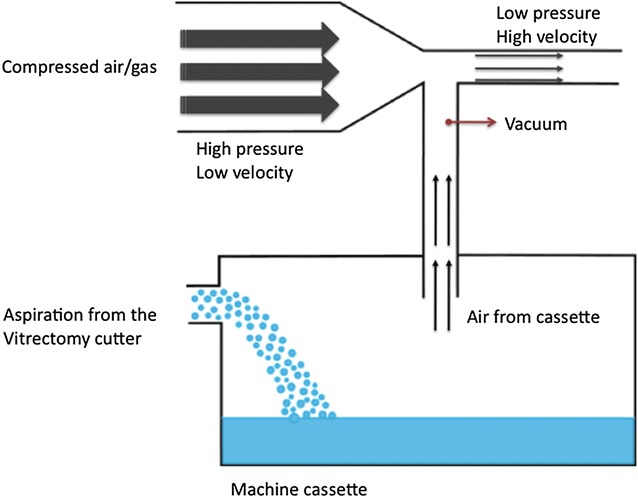
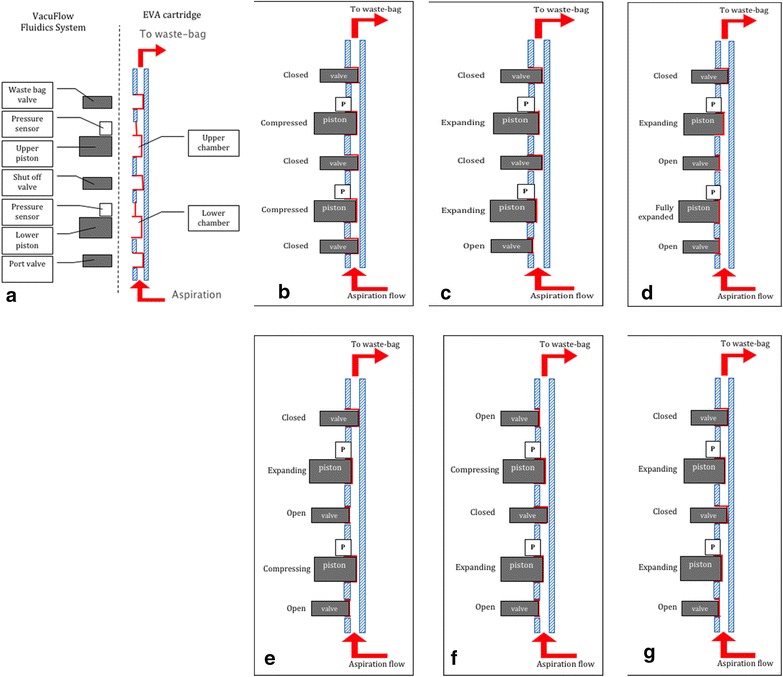
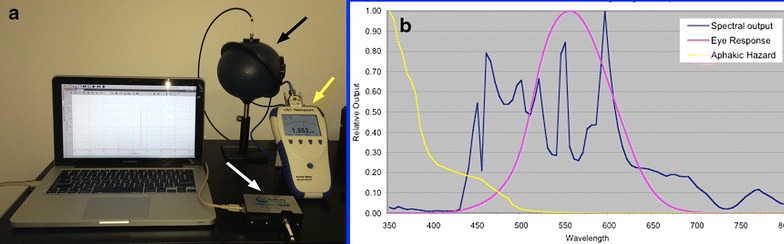
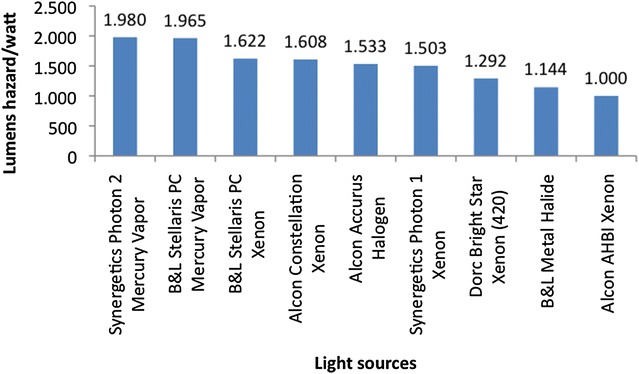
There have been many advances in vitreoretinal surgery since Machemer introduced the concept of pars plana vitrectomy, in 1971. Of particular interest are the changes in the vitrectomy cutters, their fluidics interaction, the wide-angle viewing systems and the evolution of endoillumination through the past decade and notably in the last few years. The indications of 27-gauge surgery have expanded, including more complex cases. Cut rates of up to 16,000 cuts per minute are already available. New probe designs and pump technology have allowed duty cycle performances of near 100% and improved flow control. The smaller vitrectomy diameter can be positioned between narrow spaces, allowing membrane dissection and serving as a multifunctional instrument. Enhanced endoillumination safety can be achieved by changing the light source, adding light filters, increasing the working distance and understanding the potential interactions between light and vital dyes commonly used to stain the retina. Wide-angle viewing systems (contact, non-contact or a combination of both) provide a panoramic view of the retina. Non-contact systems are assistant-independent, while contact systems may be associated with better image resolution. This review will cover some current aspects on vitrectomy procedures, mainly assessing vitrectomy cutters, as well as the importance of endoillumination and the use of wide-angle viewing systems.
Keywords: Endoillumination; Vitrectomy cutters; Wide-angle viewing systems.
Figures

References
-
- Machemer R, Buettner H, Norton EW, Parel JM. Vitrectomy: a pars plana approach. Trans Am Acad Ophthalmol Otolaryngol. 1971;75(4):813–820. - PubMed
-
- Charles S. The history of vitrectomy: innovation and evolution. Retina Today. 2008:27–9.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
