

Automated white matter fiber tract identification in patients with brain tumors
- PMID: 27981029
- PMCID: PMC5144756
- DOI: 10.1016/j.nicl.2016.11.023
Automated white matter fiber tract identification in patients with brain tumors
Abstract
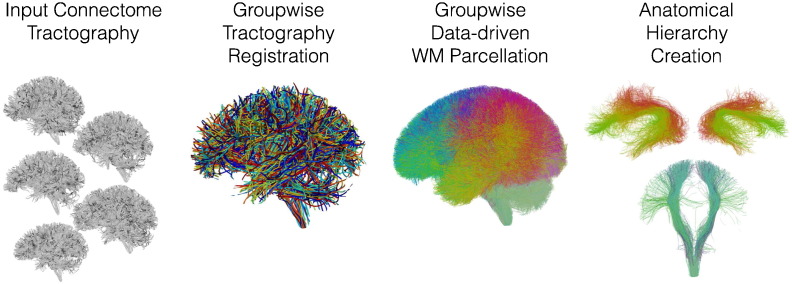
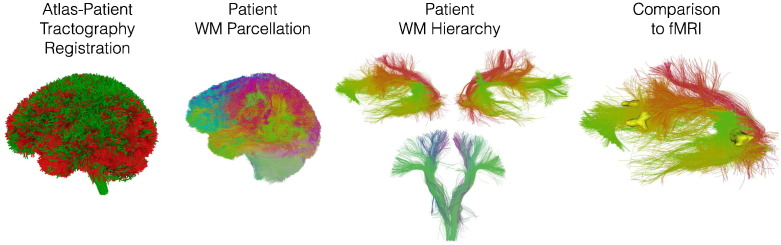
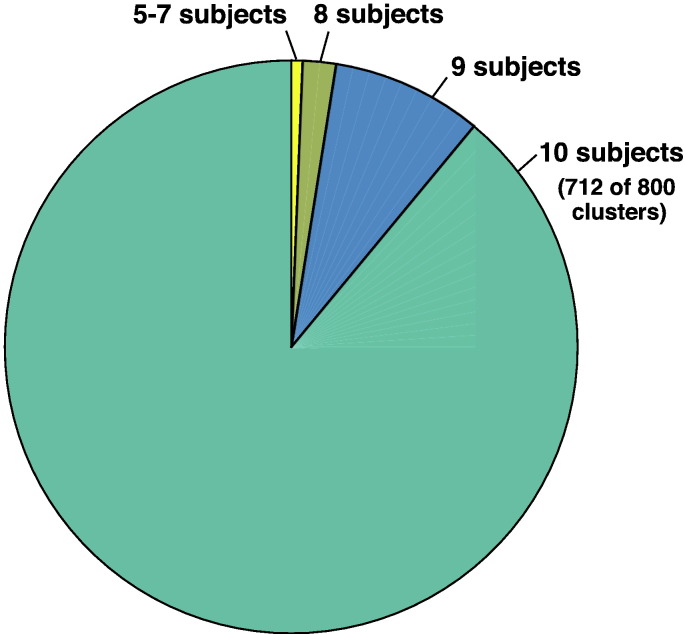
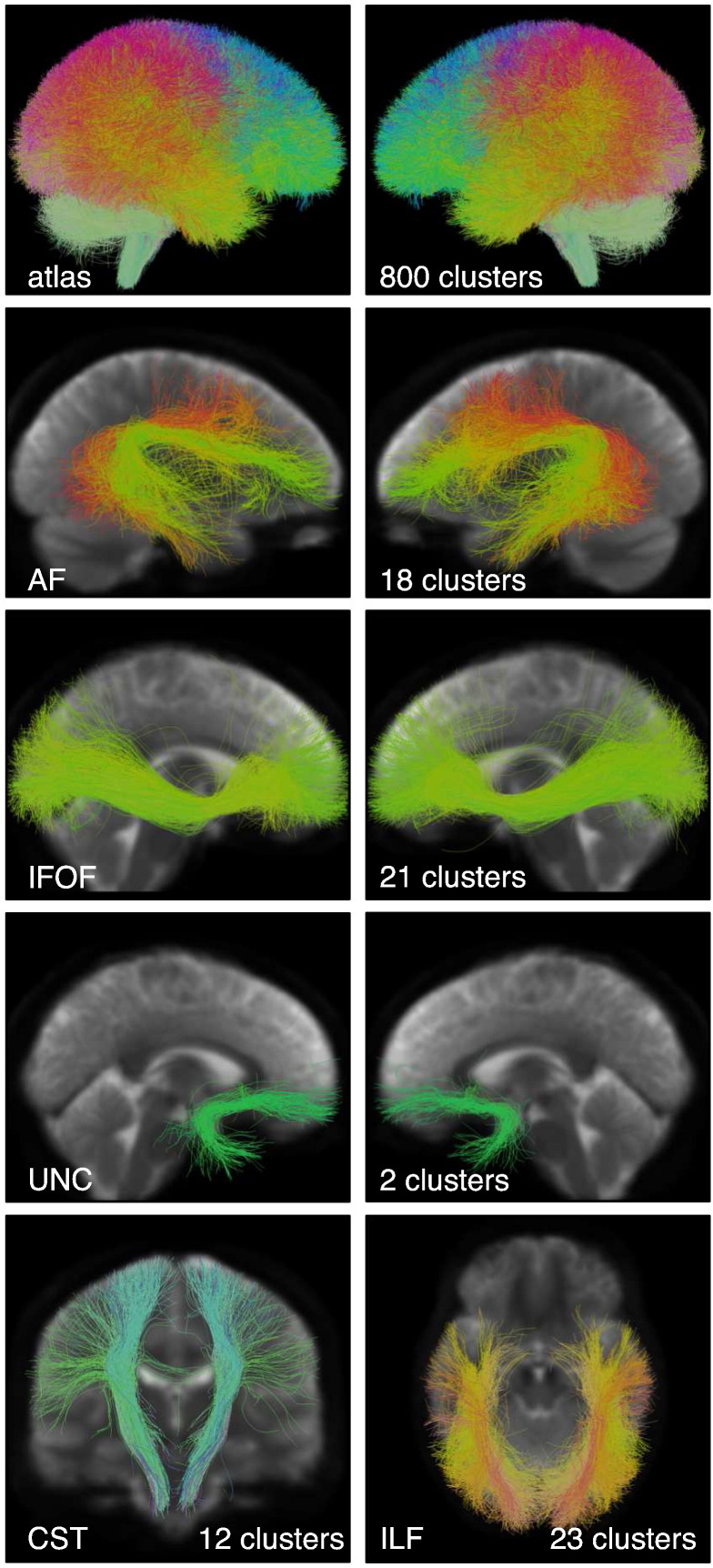
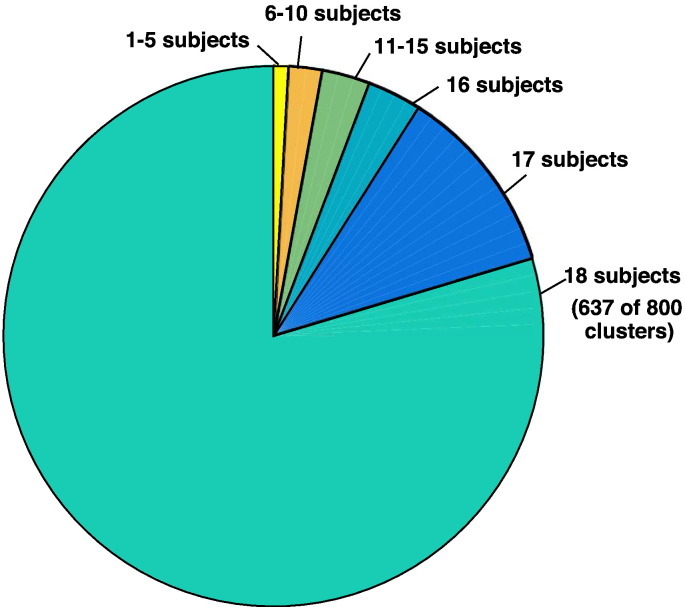
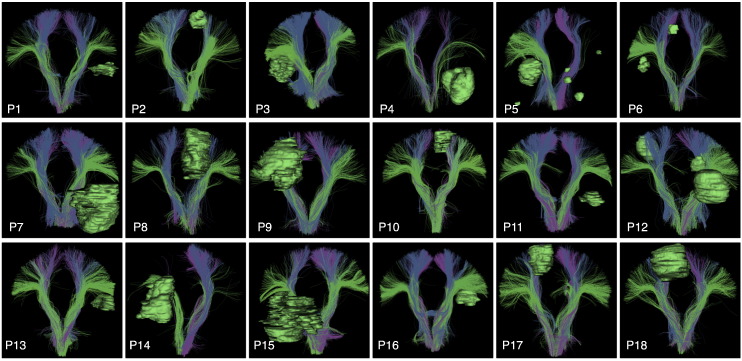
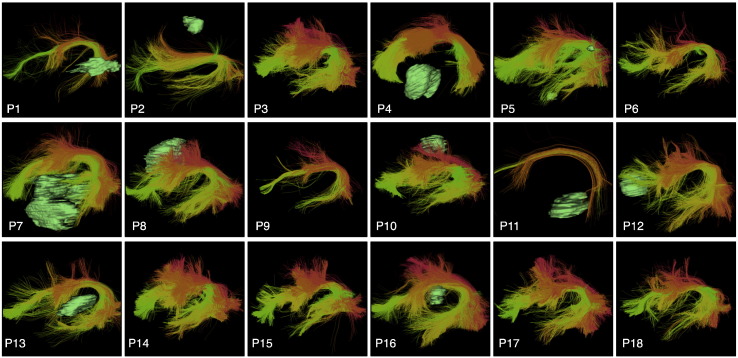
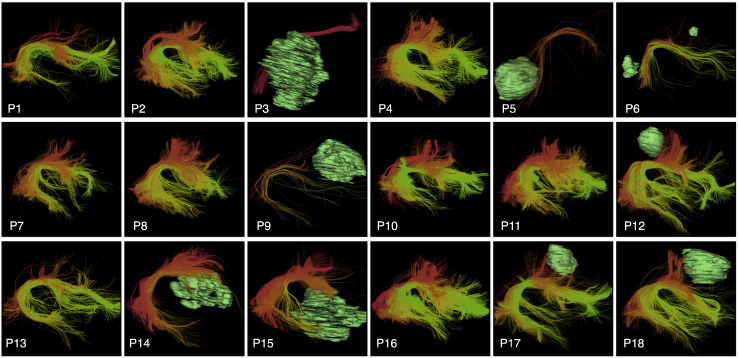
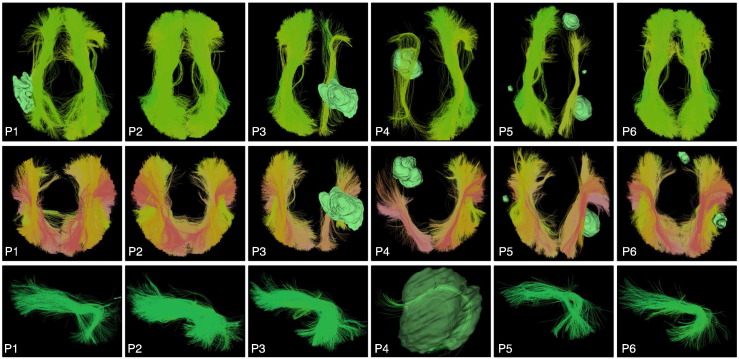
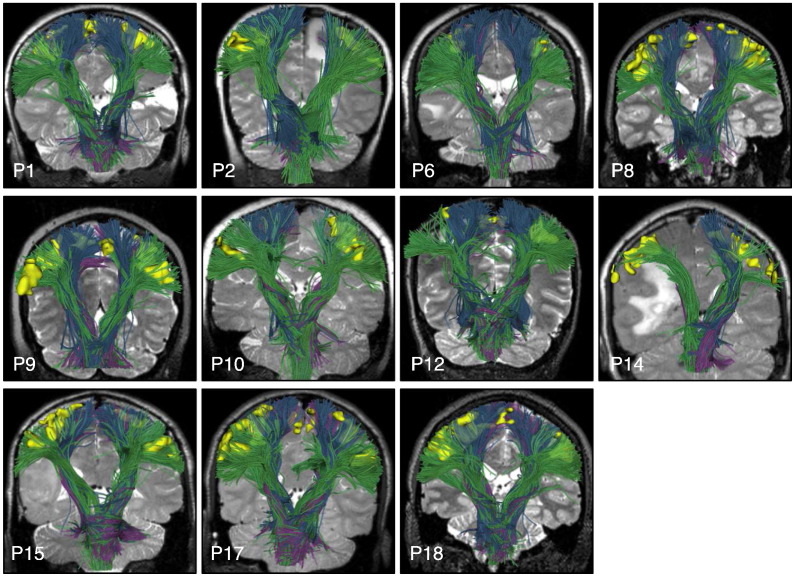
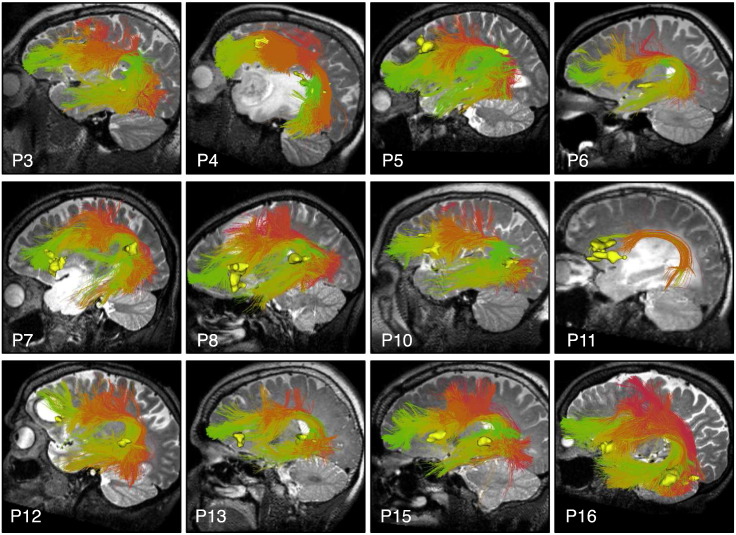
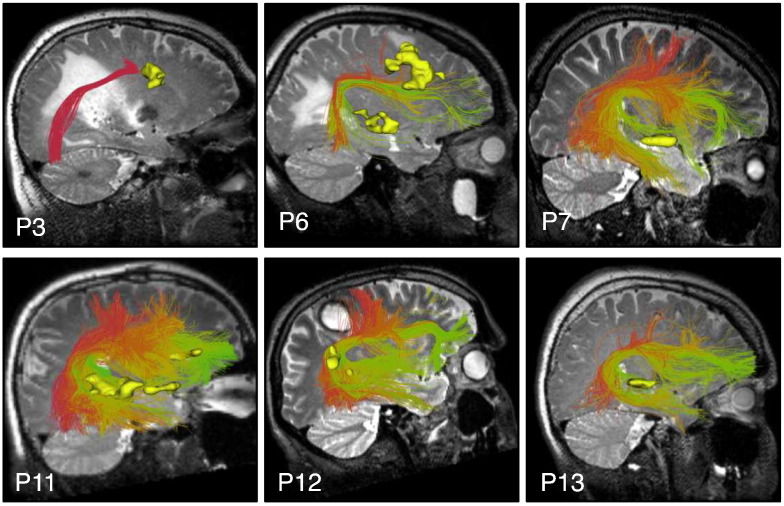
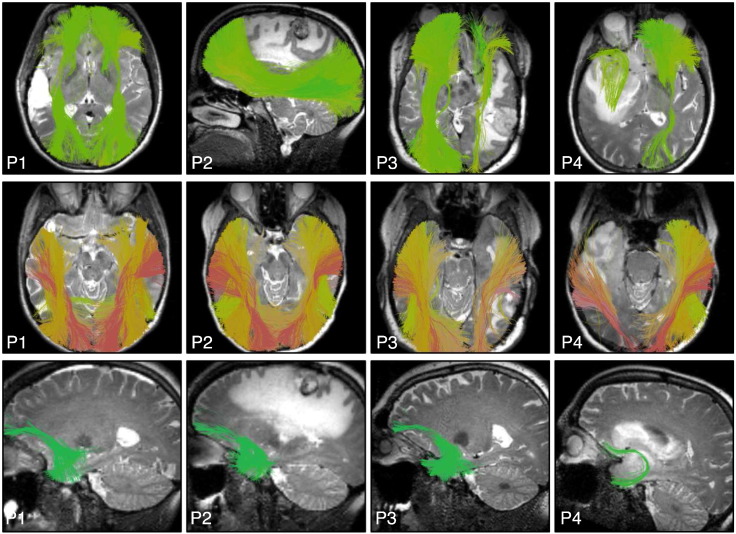
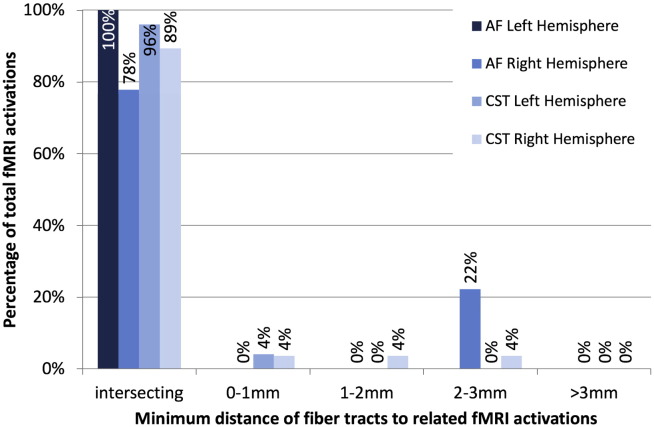
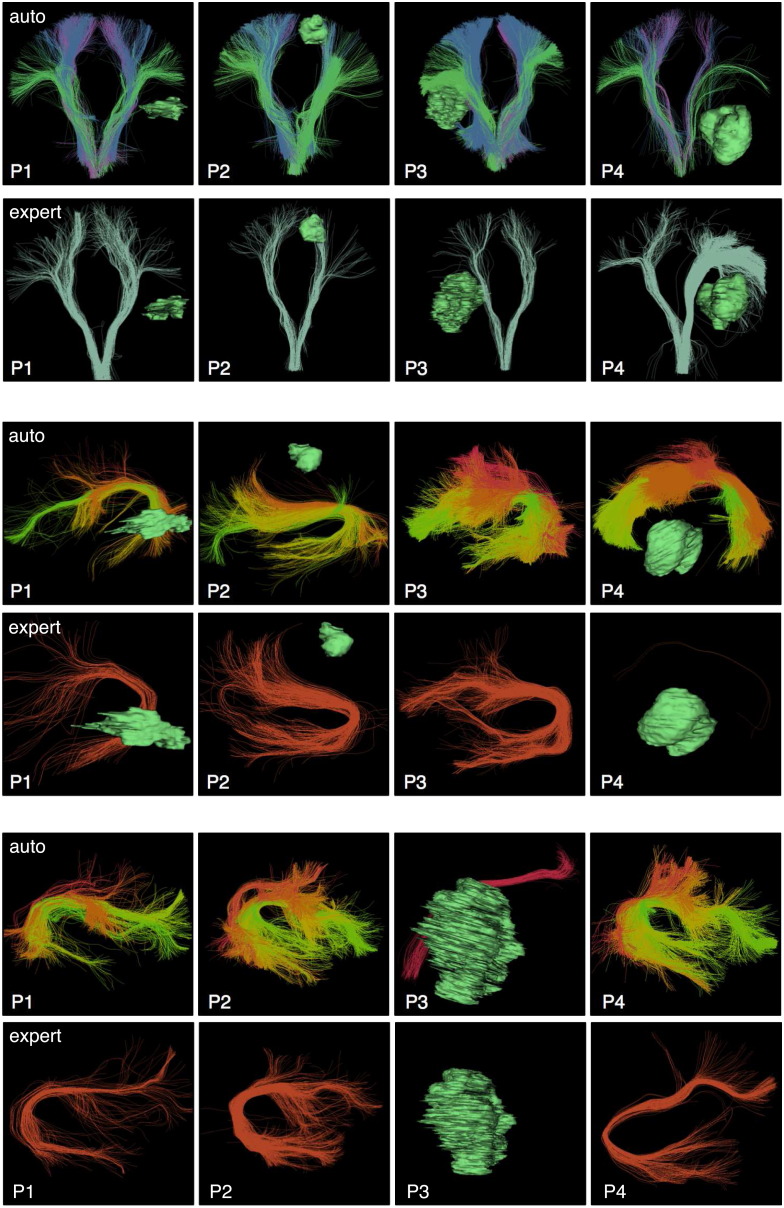
We propose a method for the automated identification of key white matter fiber tracts for neurosurgical planning, and we apply the method in a retrospective study of 18 consecutive neurosurgical patients with brain tumors. Our method is designed to be relatively robust to challenges in neurosurgical tractography, which include peritumoral edema, displacement, and mass effect caused by mass lesions. The proposed method has two parts. First, we learn a data-driven white matter parcellation or fiber cluster atlas using groupwise registration and spectral clustering of multi-fiber tractography from healthy controls. Key fiber tract clusters are identified in the atlas. Next, patient-specific fiber tracts are automatically identified using tractography-based registration to the atlas and spectral embedding of patient tractography. Results indicate good generalization of the data-driven atlas to patients: 80% of the 800 fiber clusters were identified in all 18 patients, and 94% of the 800 fiber clusters were found in 16 or more of the 18 patients. Automated subject-specific tract identification was evaluated by quantitative comparison to subject-specific motor and language functional MRI, focusing on the arcuate fasciculus (language) and corticospinal tracts (motor), which were identified in all patients. Results indicate good colocalization: 89 of 95, or 94%, of patient-specific language and motor activations were intersected by the corresponding identified tract. All patient-specific activations were within 3mm of the corresponding language or motor tract. Overall, our results indicate the potential of an automated method for identifying fiber tracts of interest for neurosurgical planning, even in patients with mass lesions.
Keywords: Diffusion MRI; Fiber tract; Neurosurgery; Tractography; Tumor; White matter.
Figures
References
-
- Al Masri O. An essay on the human corticospinal tract: history, development, anatomy, and connections. Neuroanatomy. 2011;10:1–4.
-
- Archip N., Clatz O., Whalen S., Kacher D., Fedorov A., Kot A., Chrisochoides N., Jolesz F., Golby A., Black P.M., Warfield S.K. Non-rigid alignment of pre-operative MRI, fMRI, and DT-MRI with intra-operative MRI for enhanced visualization and navigation in image-guided neurosurgery. Neuroimage. 2007;35(2):609–624. - PMC - PubMed
-
- Bastiani M., Shah N.J., Goebel R., Roebroeck A. Human cortical connectome reconstruction from diffusion weighted MRI: the effect of tractography algorithm. Neuroimage. 2012;62(3):1732–1749. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
