

Bariatric Surgery or Non-surgical Weight Loss for Idiopathic Intracranial Hypertension? A Systematic Review and Comparison of Meta-analyses
- PMID: 27981458
- PMCID: PMC5237659
- DOI: 10.1007/s11695-016-2467-7
Bariatric Surgery or Non-surgical Weight Loss for Idiopathic Intracranial Hypertension? A Systematic Review and Comparison of Meta-analyses
Abstract
Background: Idiopathic intracranial hypertension (IIH) is associated with obesity and weight loss by any means is considered beneficial in this condition.
Objectives: This study aims to appraise bariatric surgery vs. non-surgical weight-loss (medical, behavioural and lifestyle) interventions in IIH management.
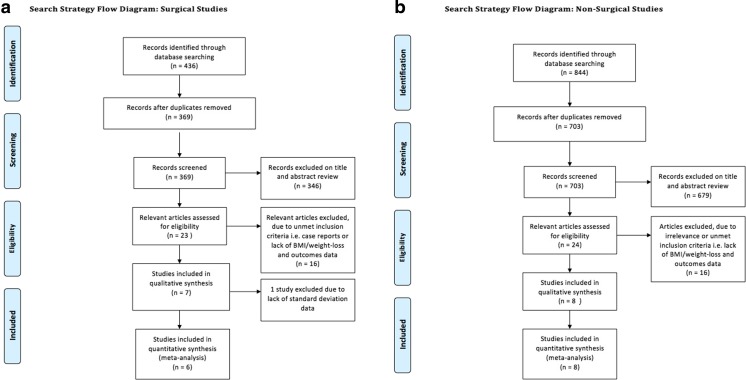
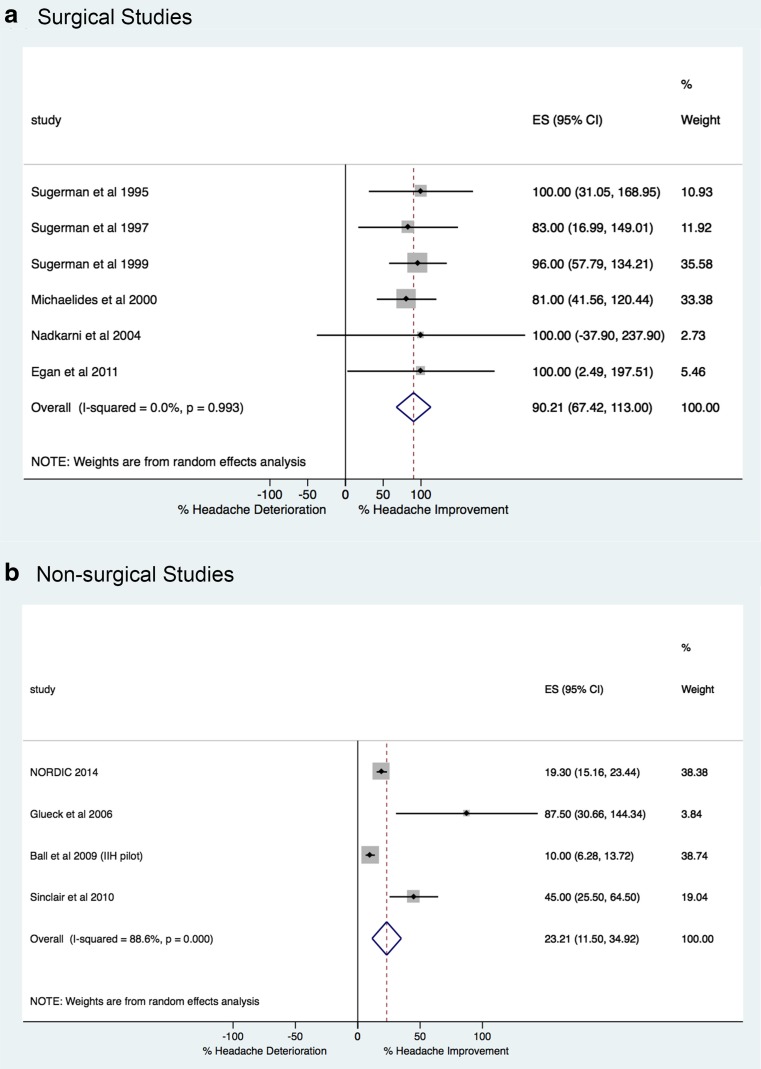
Methods: A systematic review and meta-analyses of surgical and non-surgical studies.
Results: Bariatric surgery achieved 100% papilloedema resolution and a reduction in headache symptoms in 90.2%. Non-surgical methods offered improvement in papilloedema in 66.7%, visual field defects in 75.4% and headache symptoms in 23.2%. Surgical BMI decrease was 17.5 vs. 4.2 for non-surgical methods.
Conclusions: Whilst both bariatric surgery and non-surgical weight loss offer significant beneficial effects on IIH symptomatology, future studies should address the lack of prospective and randomised trials to establish the optimal role for these interventions.
Keywords: Bariatric surgery; Benign intracranial hypertension; Idiopathic intracranial hypertension; Metabolic surgery; Obesity; Pseudotumor cerebri; Weight loss.
Conflict of interest statement
The authors have no commercial associations that might be a conflict of interest in relation to this article. Ethical Approval This article does not contain any studies with human participants or animals performed by any of the authors. Informed Consent Does not apply.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
