

Robotic salvage retroperitoneal and pelvic lymph node dissection for 'node-only' recurrent prostate cancer: technique and initial series
- PMID: 27981731
- PMCID: PMC9084626
- DOI: 10.1111/bju.13741
Robotic salvage retroperitoneal and pelvic lymph node dissection for 'node-only' recurrent prostate cancer: technique and initial series
Abstract
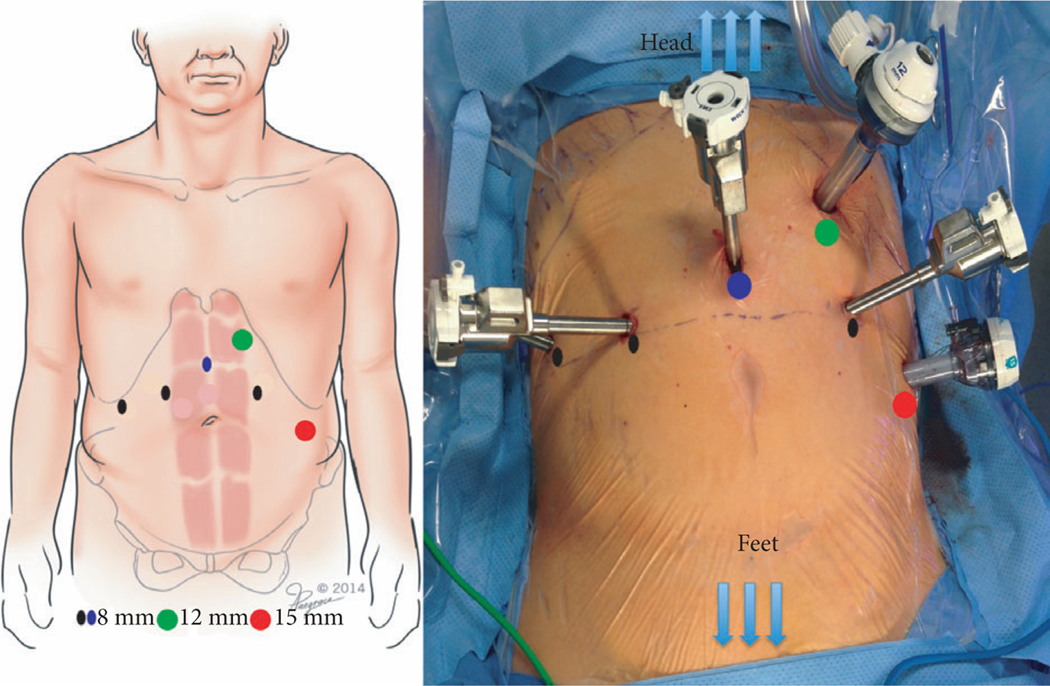
Objectives: To describe the technique of robot-assisted high-extended salvage retroperitoneal and pelvic lymphadenectomy (sRPLND+PLND) for 'node-only' recurrent prostate cancer.
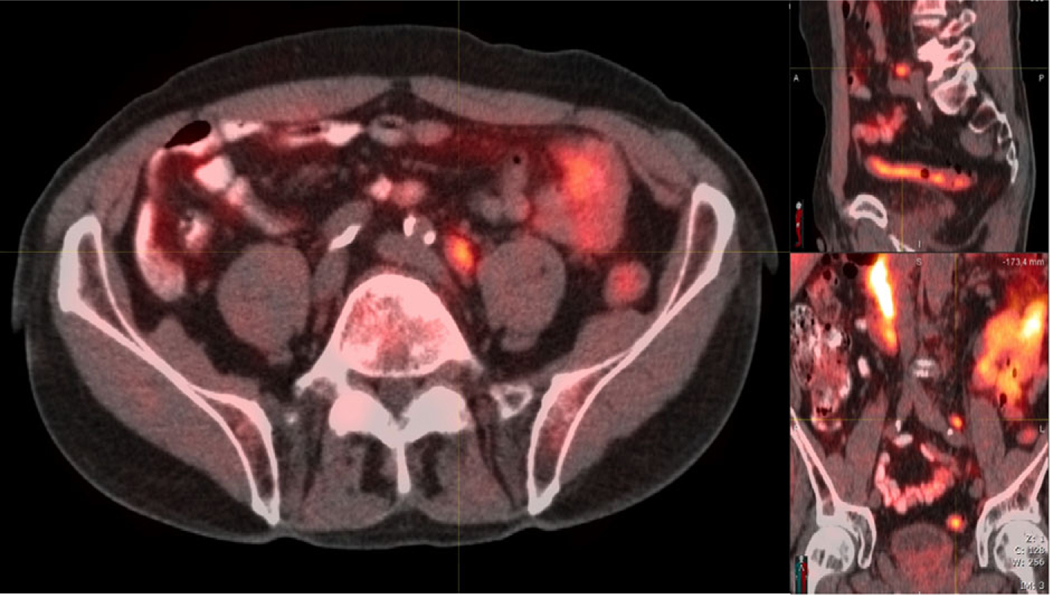
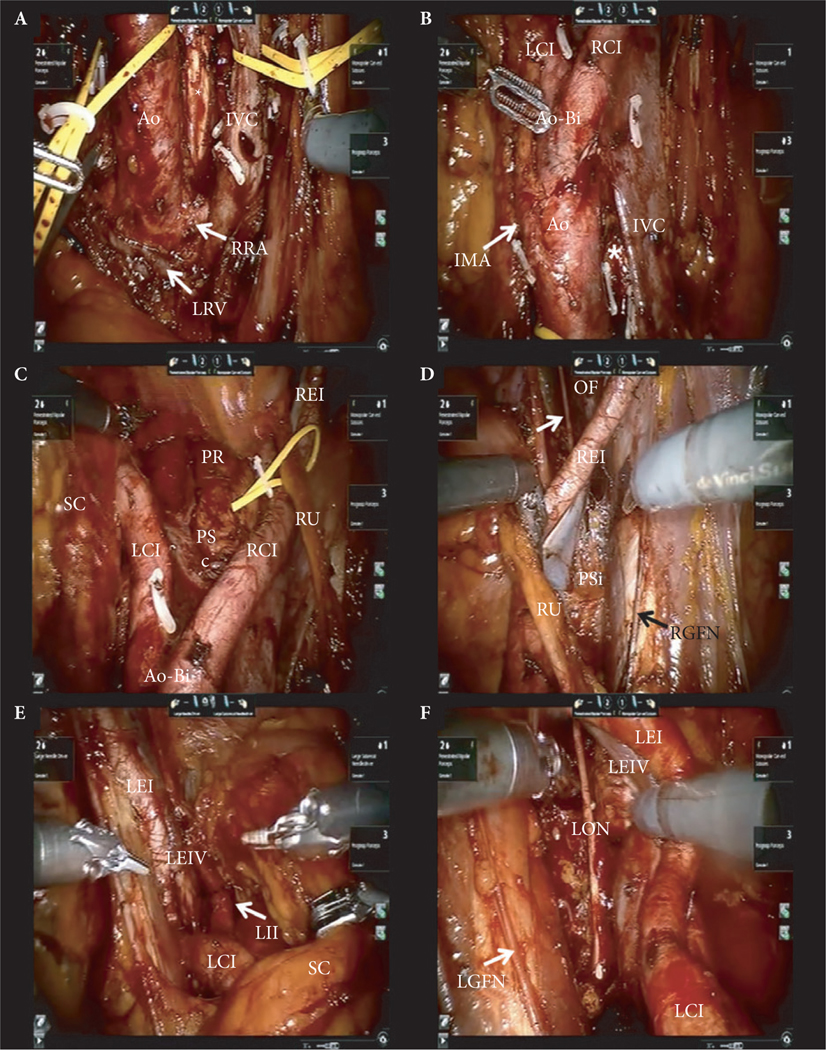
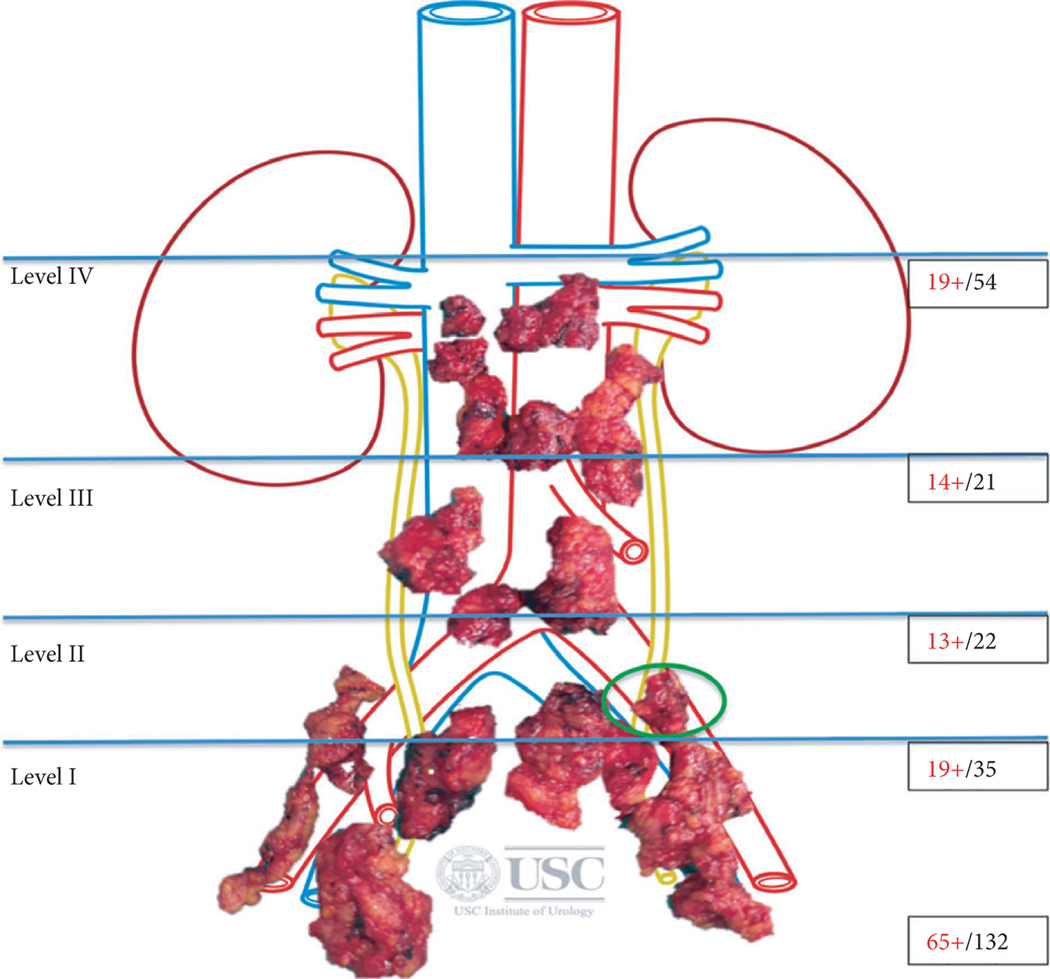
Patients and methods: In all, 10 patients underwent robot-assisted sRPLND+PLND (09/2015-03/2016) for 'node-only' recurrent prostate cancer, as identified by 11 C-acetate positron emission tomography/computed tomography imaging. Our anatomical template extends from bilateral renal artery/vein cranially up to Cloquet's node caudally, completely excising lymphatic-fatty tissue from aorto-caval and iliac vascular trees; RPLND precedes PLND. Meticulous node-mapping assessed nodes at four prospectively assigned anatomical zones.
Results: The median operative time was 4.8 h, estimated blood loss 100 mL and hospital stay 1 day. No patient had an intraoperative complication, open conversion or blood transfusion. Three patients had spontaneously resolving Clavien-Dindo grade II postoperative complications. The mean (range) number of nodes excised per patient was 83 (41-132) and mean (range) number of positive nodes per patient was 23 (0-109). Seven patients (70%) had positive nodes on final pathology. Node-positive rates per anatomical level I, II, III and IV were 28%, 32%, 33% and 33%, respectively. In patients with positive nodes, the median PSA level had decreased by 83% at the 2-month follow-up.
Conclusion: The initial series of robot-assisted sRPLND+PLND is presented, wherein we duplicate open surgery with superior nodal counts and decreased morbidity. Robot-assisted technical details for an anatomical LND template up to the renal vessels are presented. Longer follow-up is necessary to assess oncological outcomes.
Keywords: #PCSM; #ProstateCancer; robot-assisted surgery; salvage PLND; salvage RPLND.
© 2016 The Authors BJU International © 2016 BJU International Published by John Wiley & Sons Ltd.
Conflict of interest statement
Conflicts of Interest
None declared.
Figures
Comment in
-
Salvage lymph node dissection: if yes, robotics?BJU Int. 2017 Sep;120(3):304-305. doi: 10.1111/bju.13789. BJU Int. 2017. PMID: 28815976 No abstract available.
-
Re: Robotic Salvage Retroperitoneal and Pelvic Lymph Node Dissection for 'Node-Only' Recurrent Prostate Cancer: Technique and Initial Series.J Urol. 2018 Apr;199(4):875-876. doi: 10.1016/j.juro.2018.01.024. Epub 2018 Jan 17. J Urol. 2018. PMID: 29642326 No abstract available.
References
-
- Tilki D, Mandel P, Seeliger F et al. Salvage lymph node dissection for nodal recurrence of prostate cancer after radical prostatectomy. J Urol 2015; 193: 484–90 - PubMed
-
- Abdollah F, Briganti A, Montorsi F et al. Contemporary role of salvage lymphadenectomy in patients with recurrence following radical prostatectomy. Eur Urol 2015; 67: 839–49 - PubMed
-
- Jilg CA, Rischke HC, Reske SN et al. Salvage lymph node dissection with adjuvant radiotherapy for nodal recurrence of prostate cancer. J Urol 2012; 188: 2190–7 - PubMed
-
- Suardi N, Gandaglia G, Gallina A et al. Long-term outcomes of salvage lymph node dissection for clinically recurrent prostate cancer: results of a single-institution series with a minimum follow-up of 5 years. Eur Urol 2015; 67: 299–309 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
