

Evolution of multiple cell clones over a 29-year period of a CLL patient
- PMID: 27982015
- PMCID: PMC5171825
- DOI: 10.1038/ncomms13765
Evolution of multiple cell clones over a 29-year period of a CLL patient
Abstract
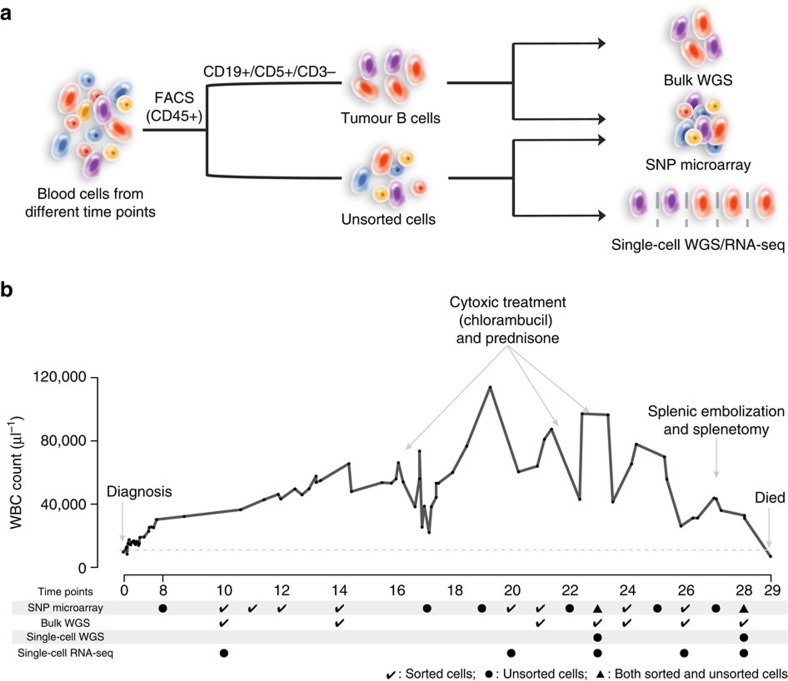
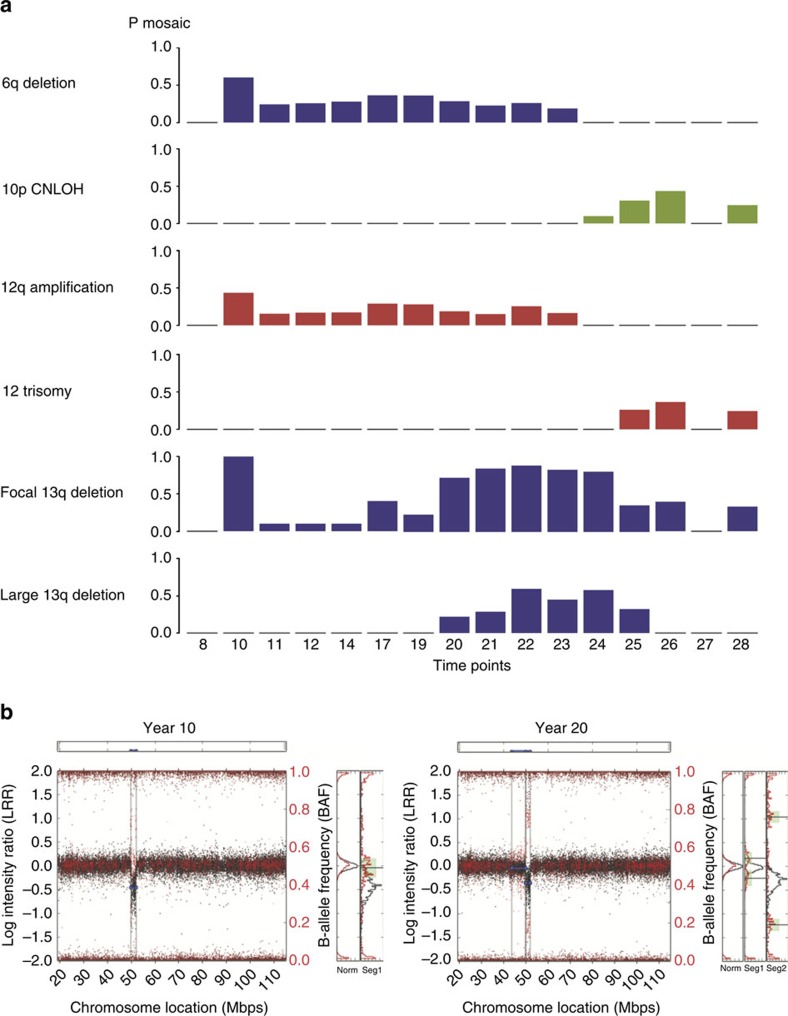
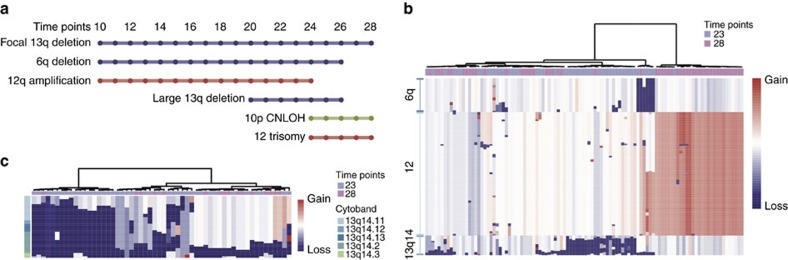
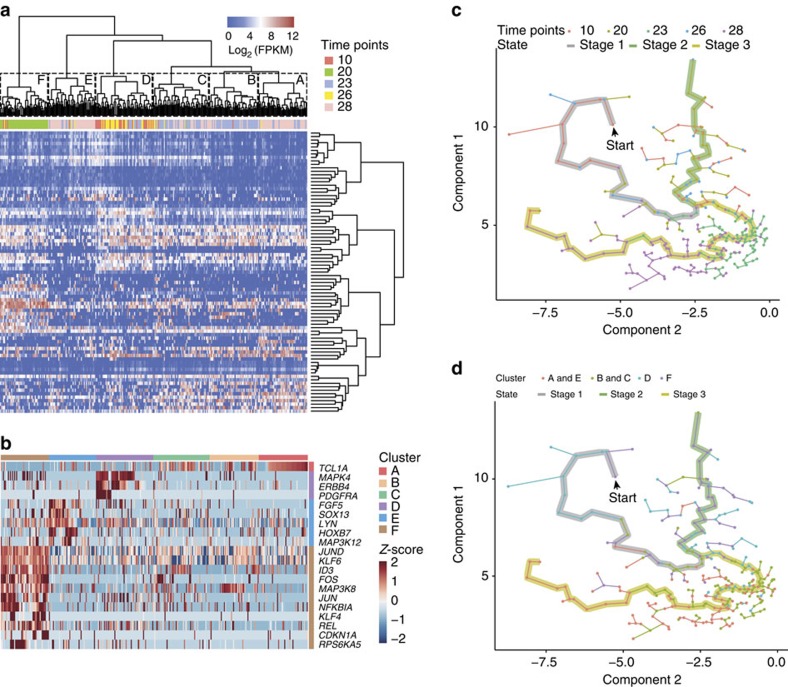
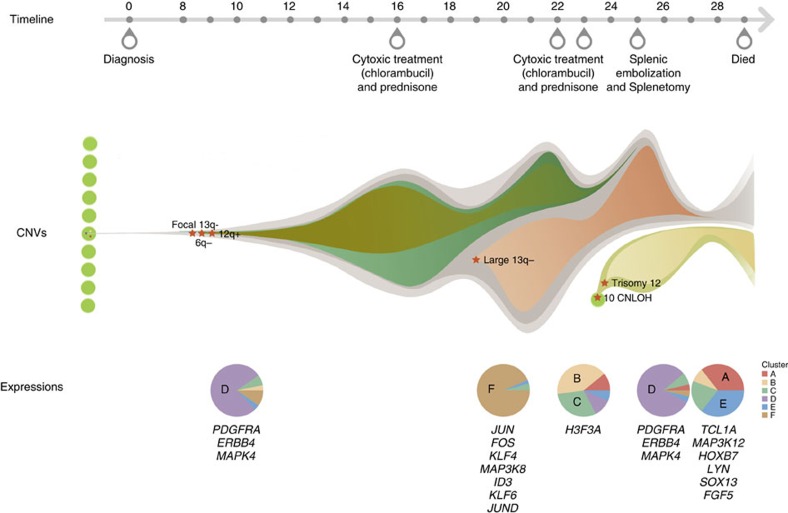
Chronic lymphocytic leukaemia (CLL) is a frequent B-cell malignancy, characterized by recurrent somatic chromosome alterations and a low level of point mutations. Here we present single-nucleotide polymorphism microarray analyses of a single CLL patient over 29 years of observation and treatment, and transcriptome and whole-genome sequencing at selected time points. We identify chromosome alterations 13q14-, 6q- and 12q+ in early cell clones, elimination of clonal populations following therapy, and subsequent appearance of a clone containing trisomy 12 and chromosome 10 copy-neutral loss of heterogeneity that marks a major population dominant at death. Serial single-cell RNA sequencing reveals an expression pattern with high FOS, JUN and KLF4 at disease acceleration, which resolves following therapy, but reoccurs following relapse and death. Transcriptome evolution indicates complex changes in expression occur over time. In conclusion, CLL can evolve gradually during indolent phases, and undergo rapid changes following therapy.
Figures
References
-
- Howlander N. et al. SEER Cancer Statistics Review, 1975–2012 (National Cancer Institute, 2015) Available at http://seer.cancer.gov/csr/1975_2012/ (2015).
-
- Siddiqi T. & Rosen S. T. Novel biologic agents for non-Hodgkin lymphoma and chronic lymphocytic leukemia-part 2: adoptive cellular immunotherapy, small-molecule inhibitors, and immunomodulation. Oncology (Williston Park) 29, 299–308 (2015). - PubMed
-
- Siddiqi T. & Rosen S. T. Novel biologic agents for non-Hodgkin lymphoma and chronic lymphocytic leukemia-part 1. Oncology (Williston Park) 29, 198–203 (2015). - PubMed
-
- Goldin L. R. & Slager S. L. Familial CLL: genes and environment. Hematology. Am. Soc. Hematol. Educ. Program 1, 339–345 (2007). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
