

Epidemiology of Hospitalizations Associated with Invasive Candidiasis, United States, 2002-20121
- PMID: 27983497
- PMCID: PMC5176241
- DOI: 10.3201/eid2301.161198
Epidemiology of Hospitalizations Associated with Invasive Candidiasis, United States, 2002-20121
Abstract
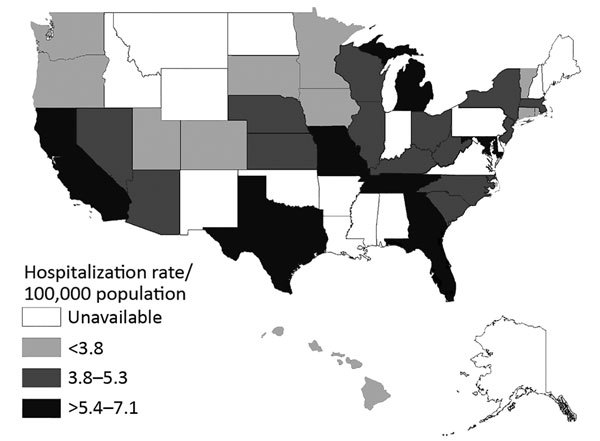
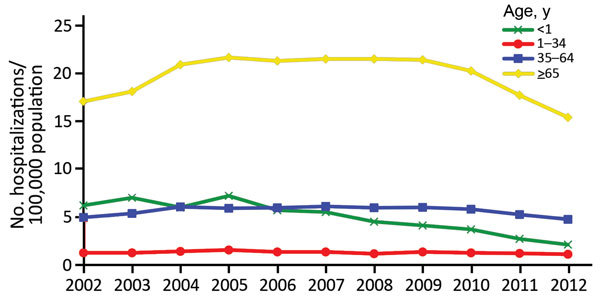
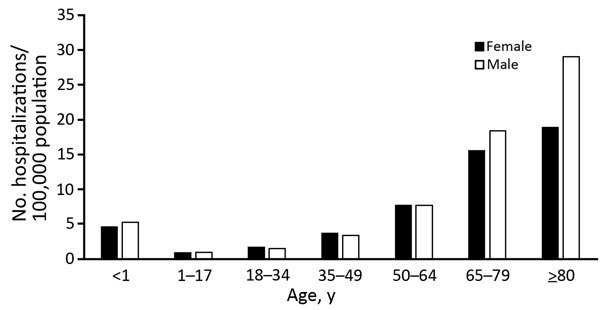
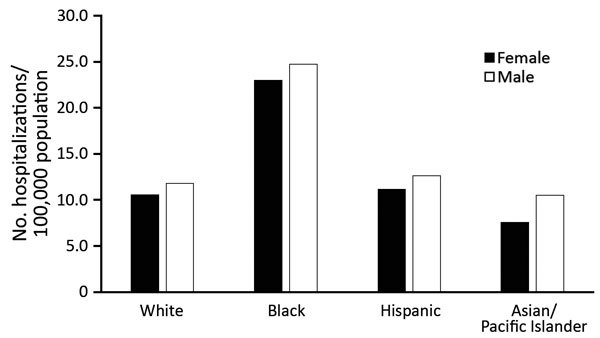
Invasive candidiasis is a major nosocomial fungal disease in the United States associated with high rates of illness and death. We analyzed inpatient hospitalization records from the Healthcare Cost and Utilization Project to estimate incidence of invasive candidiasis-associated hospitalizations in the United States. We extracted data for 33 states for 2002-2012 by using codes from the International Classification of Diseases, 9th Revision, Clinical Modification, for invasive candidiasis; we excluded neonatal cases. The overall age-adjusted average annual rate was 5.3 hospitalizations/100,000 population. Highest risk was for adults >65 years of age, particularly men. Median length of hospitalization was 21 days; 22% of patients died during hospitalization. Median unadjusted associated cost for inpatient care was $46,684. Age-adjusted annual rates decreased during 2005-2012 for men (annual change -3.9%) and women (annual change -4.5%) and across nearly all age groups. We report a high mortality rate and decreasing incidence of hospitalizations for this disease.
Keywords: Candida spp.; United States; candidemia; epidemiology; fungal infections; fungi; hospitalizations; incidence; invasive candidiasis; opportunistic infections.
Figures
References
-
- Wisplinghoff H, Ebbers J, Geurtz L, Stefanik D, Major Y, Edmond MB, et al. Nosocomial bloodstream infections due to Candida spp. in the USA: species distribution, clinical features and antifungal susceptibilities. Int J Antimicrob Agents. 2014;43:78–81. 10.1016/j.ijantimicag.2013.09.005 - DOI - PubMed
-
- Magill SS, Edwards JR, Bamberg W, Beldavs ZG, Dumyati G, Kainer MA, et al. ; Emerging Infections Program Healthcare-Associated Infections and Antimicrobial Use Prevalence Survey Team. Multistate point-prevalence survey of health care-associated infections. N Engl J Med. 2014;370:1198–208. 10.1056/NEJMoa1306801 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
