

Intraductal Tubulopapillary Neoplasm of the Pancreas: A Clinicopathologic and Immunohistochemical Analysis of 33 Cases
- PMID: 27984235
- PMCID: PMC5309137
- DOI: 10.1097/PAS.0000000000000782
Intraductal Tubulopapillary Neoplasm of the Pancreas: A Clinicopathologic and Immunohistochemical Analysis of 33 Cases
Abstract
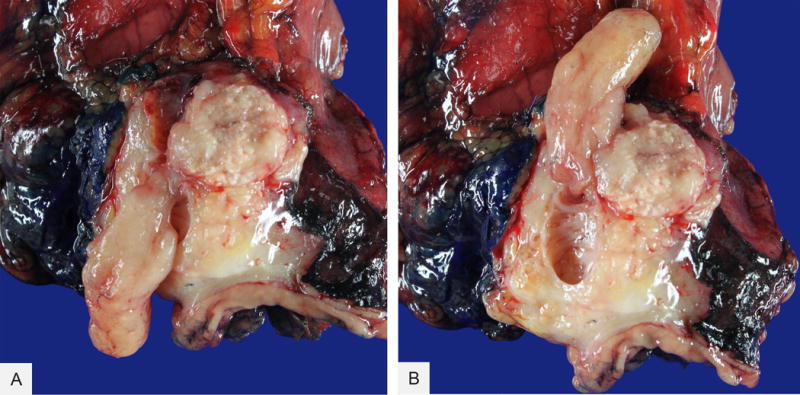
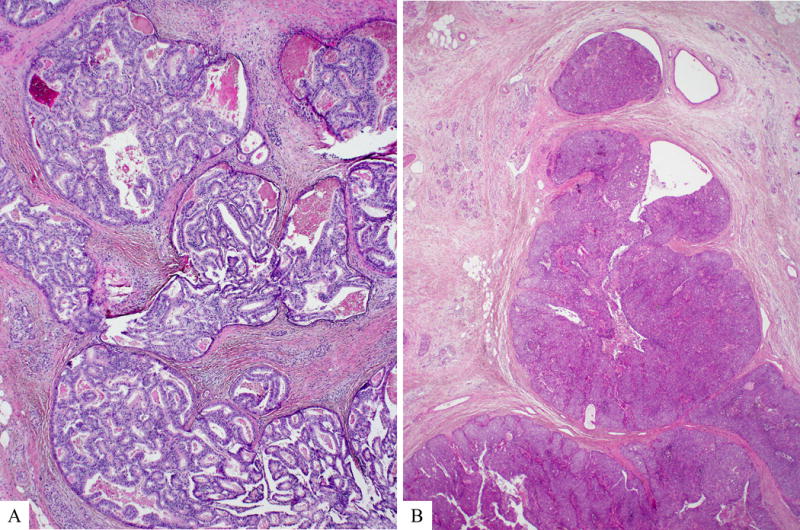
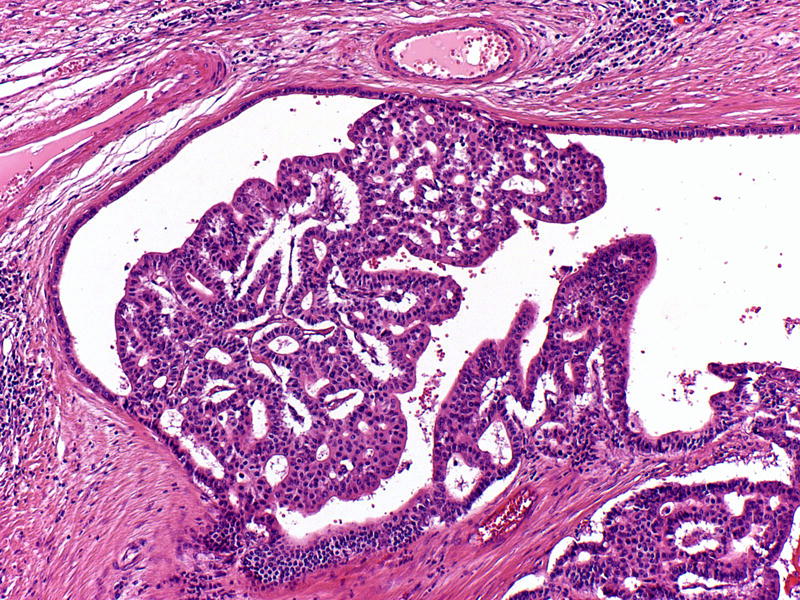
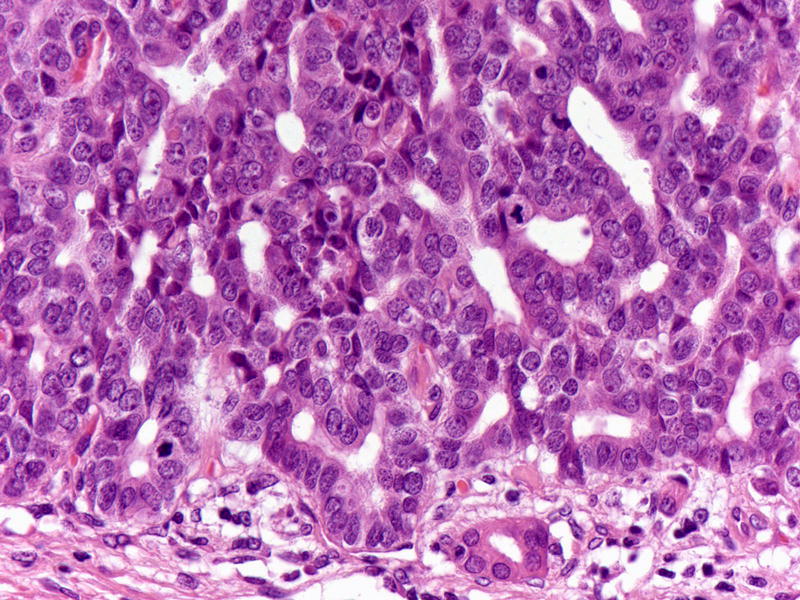
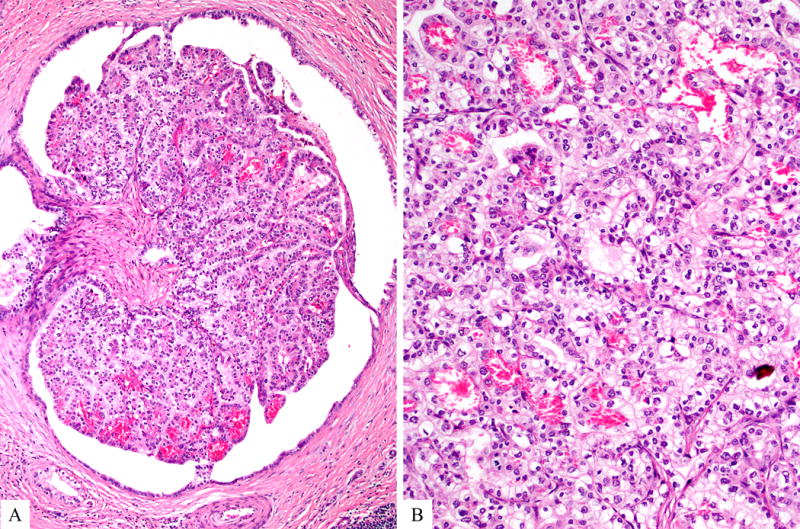
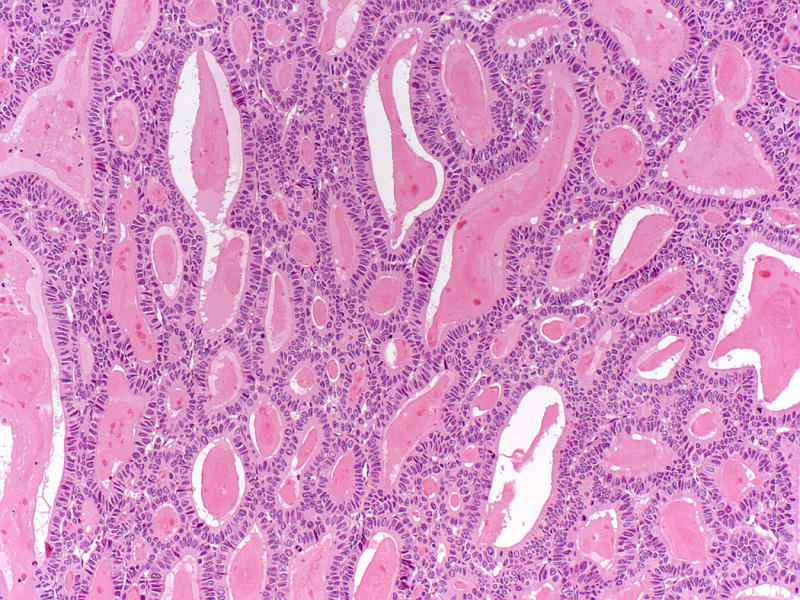
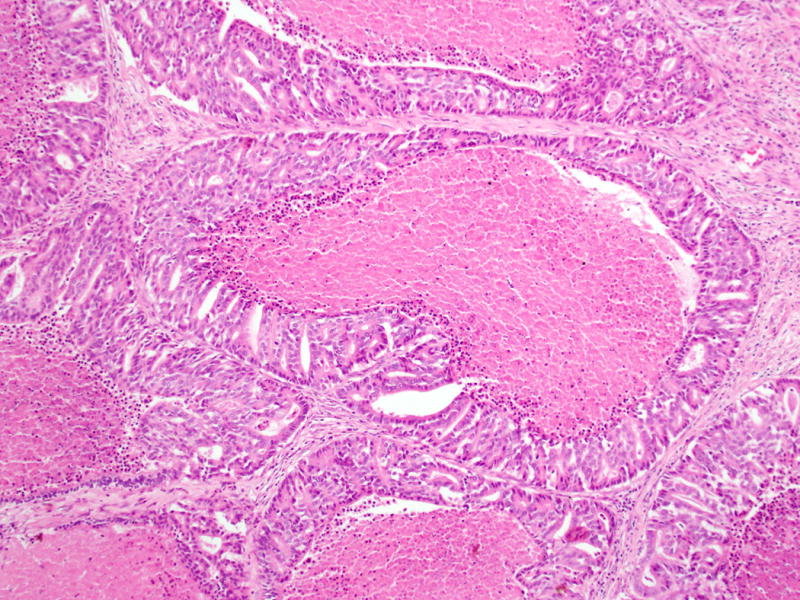
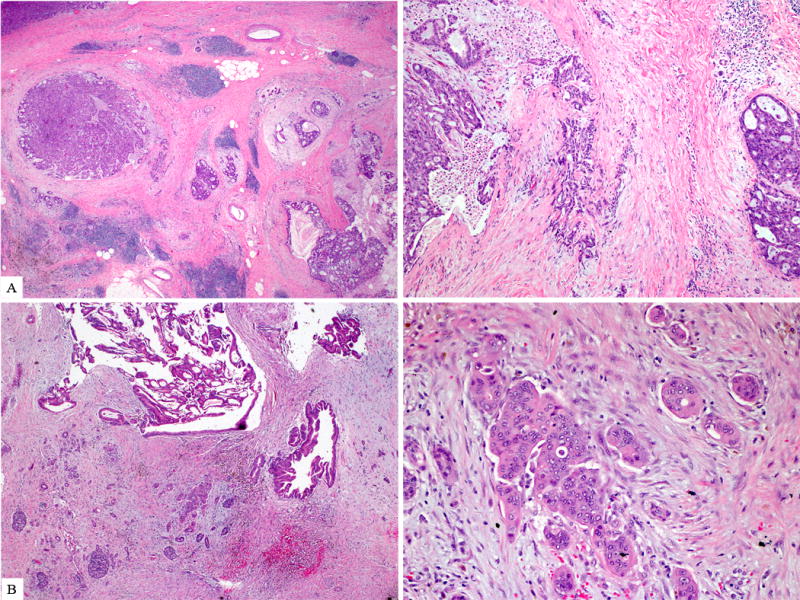
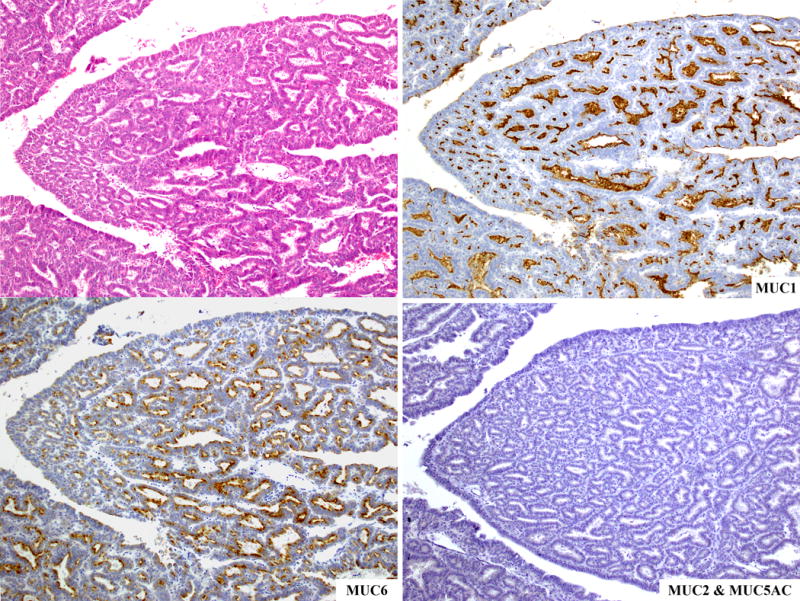
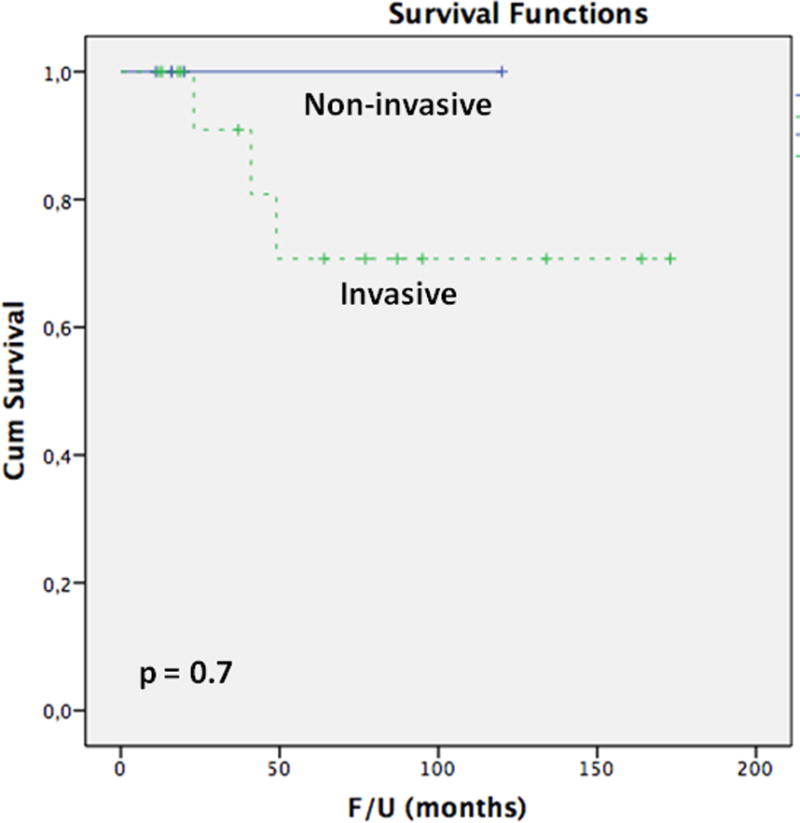
Intraductal tubulopapillary neoplasm (ITPN) is a relatively recently described member of the pancreatic intraductal neoplasm family. Thus, the literature on its histologic and immunohistochemical features, clinical behavior, and its similarities and differences from other pancreatic neoplasms is limited. Thirty-three cases of ITPN, the largest series to date, were identified. Immunohistochemical labeling for cytokeratins, glycoproteins, pancreatic enzymes, markers for intestinal and neuroendocrine differentiation, and antibodies associated with genetic alterations previously described in pancreatic neoplasms was performed. Clinicopathologic features and survival was assessed. Seventeen patients were female and 14 were male. Mean age was 55 years (range, 25 to 79 y). Median overall tumor size was 4.5 cm (range, 0.5 to 15 cm). Forty-five percent of the tumors occurred in the head, 32% in the body/tail, and 23% showed diffuse involvement. Microscopically, the tumors were characterized by intraductal nodules composed of tightly packed small tubular glands lined by cuboidal cells lacking apparent mucin. Although it was often challenging to determine its extent, invasion was present in 71%. Almost all tumors labeled for CAM5.2, CK7, and CK19; most expressed CA19.9, MUC1, and MUC6. CDX2, MUC2, trypsin, chymotrypsin, chromogranin, and synaptophysin were not expressed. SMAD4 expression was retained in 100%; p16 expression and p53 overexpression was seen in 33% and 27%, respectively. Follow-up information was available for 22 patients (median follow-up, 45 mo; range, 11 to 173 mo). Two patients with invasive carcinoma died of disease at 23 and 41 months, respectively. One patient died of unrelated causes at 49 months. Twelve patients were alive with disease. Seven patients were alive with no evidence of disease. The overall 1-, 3-, and 5-year survival rates were 100% in patients without an invasive component and 100%, 91%, and 71%, respectively, in patients with an invasive component (P=0.7). ITPN is a distinct clinicopathologic entity in the pancreas. Despite the difficulties of determining the extent of invasive carcinoma in many cases, the overall outcome seems to be relatively favorable and substantially better than that of conventional pancreatic ductal adenocarcinoma, even when only the cases with invasive carcinoma are considered.
Figures
References
-
- Ohhashi K, Murakami Y, Maruyama M. Four cases of mucous secreting pancreatic cancer. Prog Dig Endosc. 1982;20:348–351. (in Japanese, abstract in English)
-
- Adsay NV, Merati K, Basturk O, et al. Pathologically and biologically distinct types of epithelium in intraductal papillary mucinous neoplasms: delineation of an “intestinal” pathway of carcinogenesis in the pancreas. Am J Surg Pathol. 2004;28:839–48. - PubMed
-
- Hruban RH, Takaori K, Klimstra DS, et al. An illustrated consensus on the classification of pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasms. Am J Surg Pathol. 2004;28:977–87. - PubMed
-
- Furukawa T, Kloppel G, Volkan Adsay N, et al. Classification of types of intraductal papillary-mucinous neoplasm of the pancreas: a consensus study. Virchows Arch. 2005;447:794–9. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
