

Morphologic Features of Magnetic Resonance Imaging as a Surrogate of Capsular Contracture in Breast Cancer Patients With Implant-based Reconstructions
- PMID: 27986345
- PMCID: PMC5541677
- DOI: 10.1016/j.ijrobp.2016.09.041
Morphologic Features of Magnetic Resonance Imaging as a Surrogate of Capsular Contracture in Breast Cancer Patients With Implant-based Reconstructions
Abstract
Purpose: Capsular contracture (CC) is a serious complication in patients receiving implant-based reconstruction for breast cancer. Currently, no objective methods are available for assessing CC. The goal of the present study was to identify image-based surrogates of CC using magnetic resonance imaging (MRI).
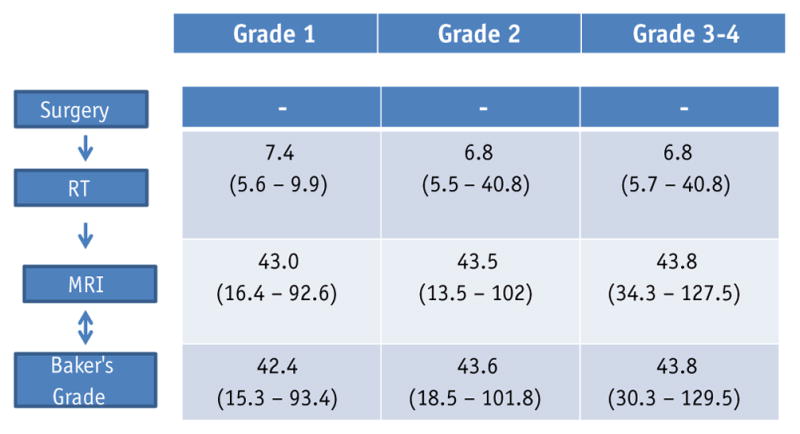
Methods and materials: We analyzed a retrospective data set of 50 patients who had undergone both a diagnostic MRI scan and a plastic surgeon's evaluation of the CC score (Baker's score) within a 6-month period after mastectomy and reconstructive surgery. The MRI scans were assessed for morphologic shape features of the implant and histogram features of the pectoralis muscle. The shape features, such as roundness, eccentricity, solidity, extent, and ratio length for the implant, were compared with the Baker score. For the pectoralis muscle, the muscle width and median, skewness, and kurtosis of the intensity were compared with the Baker score. Univariate analysis (UVA) using a Wilcoxon rank-sum test and multivariate analysis with the least absolute shrinkage and selection operator logistic regression was performed to determine significant differences in these features between the patient groups categorized according to their Baker's scores.
Results: UVA showed statistically significant differences between grade 1 and grade ≥2 for morphologic shape features and histogram features, except for volume and skewness. Only eccentricity, ratio length, and volume were borderline significant in differentiating grade ≤2 and grade ≥3. Features with P<.1 on UVA were used in the multivariate least absolute shrinkage and selection operator logistic regression analysis. Multivariate analysis showed a good level of predictive power for grade 1 versus grade ≥2 CC (area under the receiver operating characteristic curve 0.78, sensitivity 0.78, and specificity 0.82) and for grade ≤2 versus grade ≥3 CC (area under the receiver operating characteristic curve 0.75, sensitivity 0.75, and specificity 0.79).
Conclusions: The morphologic shape features described on MR images were associated with the severity of CC. MRI has the potential to further improve the diagnostic ability of the Baker score in breast cancer patients who undergo implant reconstruction.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest: none.
Figures




Similar articles
-
A Phase II Study Evaluating the Effect of Intensity Modulated Postmastectomy Radiation Therapy on Implant Failure Rates in Breast Cancer Patients With Immediate, 2-Stage Implant Reconstruction With an MRI Imaging Correlative Substudy.Int J Radiat Oncol Biol Phys. 2024 Oct 1;120(2):482-495. doi: 10.1016/j.ijrobp.2024.03.031. Epub 2024 Apr 2. Int J Radiat Oncol Biol Phys. 2024. PMID: 38570168 Clinical Trial.
-
Objective assessment of reconstructed breast hardness using a durometer.Breast Cancer. 2018 Jan;25(1):81-85. doi: 10.1007/s12282-017-0791-y. Epub 2017 Jun 23. Breast Cancer. 2018. PMID: 28646371
-
Imaging of breast implant and implant-associated complications: Capsular contracture and intra- or extracapsular rupture.Clin Hemorheol Microcirc. 2020;76(2):221-231. doi: 10.3233/CH-209218. Clin Hemorheol Microcirc. 2020. PMID: 32925022
-
A review of the literature on the etiology of capsular contracture and a pilot study to determine the outcome of capsular contracture interventions.Aesthetic Plast Surg. 1999 May-Jun;23(3):197-206. doi: 10.1007/s002669900268. Aesthetic Plast Surg. 1999. PMID: 10384019 Review.
-
[Radiotherapy and breast reconstruction: the issue of compatibility].Orv Hetil. 2003 Mar 23;144(12):549-55. Orv Hetil. 2003. PMID: 12723525 Review. Hungarian.
Cited by
-
Assessment of Capsular Contracture Based on Morphological Change of Breast Implant Using Computed Tomography.Arch Plast Surg. 2025 Jul 23;52(4):217-224. doi: 10.1055/a-2620-3350. eCollection 2025 Jul. Arch Plast Surg. 2025. PMID: 40709003 Free PMC article.
-
Ultrasound Criteria and Baker Scale for Breast Implant Capsular Contracture Diagnosis.Plast Reconstr Surg Glob Open. 2022 Oct 19;10(10):e4582. doi: 10.1097/GOX.0000000000004582. eCollection 2022 Oct. Plast Reconstr Surg Glob Open. 2022. PMID: 36284718 Free PMC article.
-
A Phase II Study Evaluating the Effect of Intensity Modulated Postmastectomy Radiation Therapy on Implant Failure Rates in Breast Cancer Patients With Immediate, 2-Stage Implant Reconstruction With an MRI Imaging Correlative Substudy.Int J Radiat Oncol Biol Phys. 2024 Oct 1;120(2):482-495. doi: 10.1016/j.ijrobp.2024.03.031. Epub 2024 Apr 2. Int J Radiat Oncol Biol Phys. 2024. PMID: 38570168 Clinical Trial.
-
An experimental study on the prosthesis produced by inactivated autologous subcutaneous adipose tissue and skin dermal tissue in a mini-pig model.Transl Cancer Res. 2020 Aug;9(8):4770-4780. doi: 10.21037/tcr-19-2844. Transl Cancer Res. 2020. PMID: 35117840 Free PMC article.
-
Toward a Consensus Aproach for Assessing Capsular Contracture Severity and Progression: A Systematic Review.Plast Reconstr Surg. 2024 Jan 1;153(1):7-22. doi: 10.1097/PRS.0000000000010573. Epub 2023 Apr 20. Plast Reconstr Surg. 2024. PMID: 37075286 Free PMC article.
References
-
- Gabriel SE, Woods JE, O’Fallon WM, et al. Complications leading to surgery after breast implantation. N Engl J Med. 1997;336:677–682. - PubMed
-
- Embrey M, Adams EE, Cunningham B, et al. A review of the literature on the etiology of capsular contracture and a pilot study to determine the outcome of capsular contracture interventions. Aesthetic Plast Surg. 1999;23:197–206. - PubMed
-
- Coleman DJ, Sharpe DT, Naylor IL, et al. The role of the contractile fibroblast in the capsules around tissue expanders and implants. Br J Plast Surg. 1993;46:547–556. - PubMed
-
- Piscatelli SJ, Partington M, Hobar C, et al. Breast capsule contracture: Is fibroblast activity associated with severity? Aesthetic Plast Surg. 1994;18:75–79. - PubMed
-
- Rubino C, Mazzarello V, Farace F, et al. Ultrastructural anatomy of contracted capsules around textured implants in augmented breasts. Ann Plast Surg. 2001;46:95–102. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
