

Country-Level Cost-Effectiveness Thresholds: Initial Estimates and the Need for Further Research
- PMID: 27987642
- PMCID: PMC5193154
- DOI: 10.1016/j.jval.2016.02.017
Country-Level Cost-Effectiveness Thresholds: Initial Estimates and the Need for Further Research
Abstract
Background: Cost-effectiveness analysis can guide policymakers in resource allocation decisions. It assesses whether the health gains offered by an intervention are large enough relative to any additional costs to warrant adoption. When there are constraints on the health care system's budget or ability to increase expenditures, additional costs imposed by interventions have an "opportunity cost" in terms of the health foregone because other interventions cannot be provided. Cost-effectiveness thresholds (CETs) are typically used to assess whether an intervention is worthwhile and should reflect health opportunity cost. Nevertheless, CETs used by some decision makers-such as the World Health Organization that suggested CETs of 1 to 3 times the gross domestic product (GDP) per capita-do not.
Objectives: To estimate CETs based on opportunity cost for a wide range of countries.
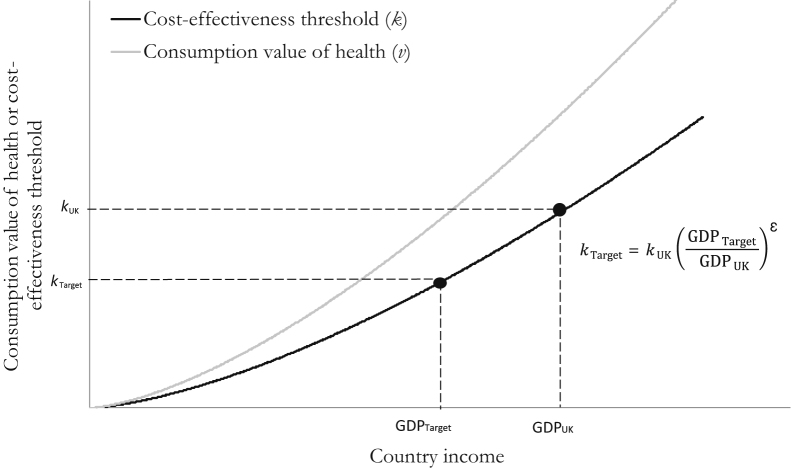
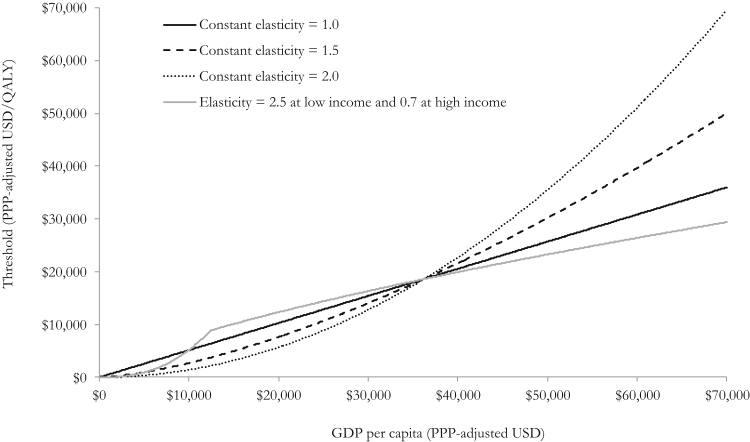
Methods: We estimated CETs based on recent empirical estimates of opportunity cost (from the English National Health Service), estimates of the relationship between country GDP per capita and the value of a statistical life, and a series of explicit assumptions.
Results: CETs for Malawi (the country with the lowest income in the world), Cambodia (with borderline low/low-middle income), El Salvador (with borderline low-middle/upper-middle income), and Kazakhstan (with borderline high-middle/high income) were estimated to be $3 to $116 (1%-51% GDP per capita), $44 to $518 (4%-51%), $422 to $1967 (11%-51%), and $4485 to $8018 (32%-59%), respectively.
Conclusions: To date, opportunity-cost-based CETs for low-/middle-income countries have not been available. Although uncertainty exists in the underlying assumptions, these estimates can provide a useful input to inform resource allocation decisions and suggest that routinely used CETs have been too high.
Keywords: benefits package; cost-effectiveness; quality-adjusted life-years; threshold; universal health care; willingness to pay.
Copyright © 2016 International Society for Pharmacoeconomics and Outcomes Research (ISPOR). Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Drummond M.F., Sculpher M.J., Claxton K. Evaluation of Health Care Programmes. 4th ed.) Oxford University Press; Oxford, UK: 2015. Methods for the Economic.
-
- Claxton K, Walker S, Palmer S, Sculpher M. Appropriate perspectives for health care decisions. CHE Research Paper 54, Centre for Health Economics, University of York, 2010.
-
- Claxton K, Martin S, Soares M, et al. Methods for the estimation of the NICE cost-effectiveness threshold. CHE Research Paper 81, Centre for Health Economics, University of York, 2013.
-
- Neumann P.J., Cohen J.T., Weinstein M.C. Updating cost-effectiveness—the curious resilience of the $50,000-per-QALY threshold. N Engl J Med. 2014;371:796–797. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25692211. [Accessed December 2014] - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
