

The effect of surgeon and hospital volume on mortality after open and endovascular repair of abdominal aortic aneurysms
- PMID: 27988158
- PMCID: PMC5329005
- DOI: 10.1016/j.jvs.2016.09.036
The effect of surgeon and hospital volume on mortality after open and endovascular repair of abdominal aortic aneurysms
Abstract
Background: Higher hospital and surgeon volumes are independently associated with improved mortality after open repair of abdominal aortic aneurysms (AAAs) in the era before endovascular AAA repair (EVAR). The effects of both surgeon and hospital volume on mortality after EVAR and open repair in the current era are less well defined.
Methods: We studied Medicare beneficiaries who underwent elective AAA repair from 2001 to 2008. Volume was measured by procedure type during the 1-year period preceding each procedure and was further categorized into quintiles of volume for surgeon and hospital. Multilevel logistic regression models were used to evaluate the effect of surgeon volume, accounting for hospital volume, on mortality after adjusting for patient demographic and comorbid conditions as well as the analogous effect of hospital volume adjusting for surgeon volume. The multilevel models included random effects for surgeon and hospital to account for the clustering of multiple patients within the same surgeon and within the same hospital.
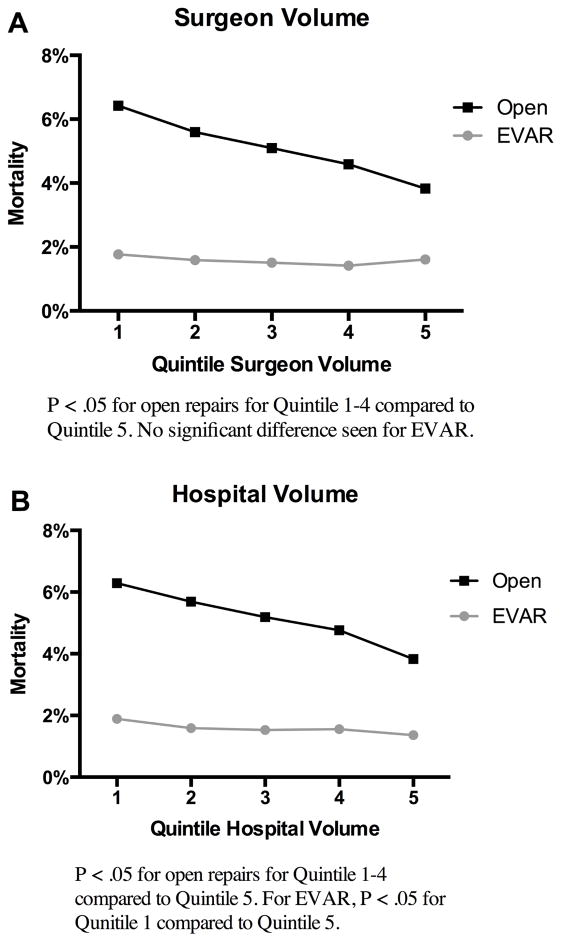
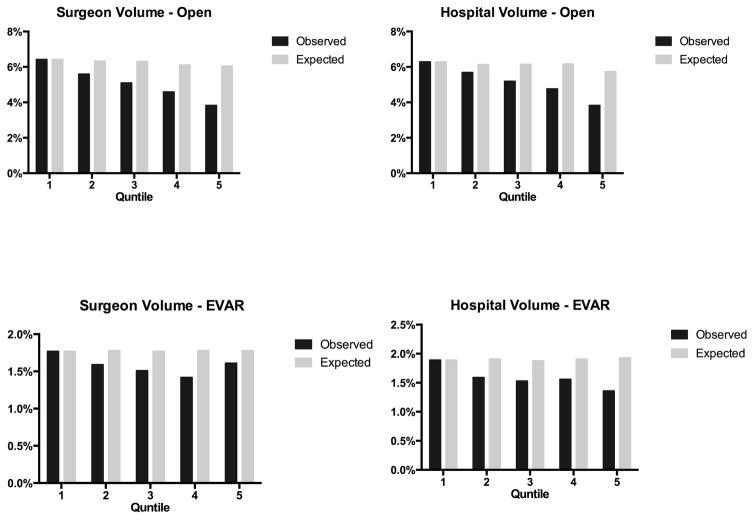
Results: We studied 122,495 patients who underwent AAA repair (open: 45,451; EVAR: 77,044). After EVAR, perioperative mortality did not differ by surgeon volume (quintile 1 [0-6 EVARs]: 1.8%; quintile 5 [28-151 EVARs]: 1.6%; P = .29), but decreased with greater hospital volume (quintile 1 [0-9 EVARs]: 1.9%; quintile 5 [49-198 EVARs]: 1.4%; P < .01). After open repair, perioperative mortality decreased with both higher surgeon volume (quintile 1 [0-3 open repairs]: 6.4%; quintile 5 [14-62 open repairs]: 3.8%; P < .01) and hospital volume (quintile 1 [0-5 open repairs]: 6.3%; quintile 5 [14-62 open repairs]: 3.8%; P < .01). After adjustment for other predictors, surgeon volume was not associated with perioperative mortality after EVAR (odds ratio [OR], 0.9; 95% confidence interval [CI], 0.7-1.1); however, hospital volume was associated with higher perioperative mortality (quintile 1: OR, 1.5; 95% CI, 1.2-1.9; quintile 2: OR, 1.3; 95% CI, 1.02-1.6; and quintile 3: OR, 1.2; 95% CI, 1.01-1.5, compared with 5). After open repair, higher surgeon volume was also associated with lower mortality (quintile 1: OR, 1.5; 95% CI, 1.3-1.8; quintile 2: OR, 1.3; 95% CI, 1.1-1.6; and quintile 3: OR, 1.2; 95% CI, 1.1-1.4, compared with 5). Risk of mortality also was higher for patients treated at lower-volume hospitals (quintile 1: OR, 1.3; 95% CI, 1.1-1.5; quintile 2: OR, 1.3; 95% CI, 1.1-1.5; and quintile 3: OR, 1.2; 95% CI, 1.1-1.4, compared with 5).
Conclusions: After EVAR, hospital volume is minimally associated with perioperative mortality, with no such association for surgeon volume. After open AAA repair, surgeon and hospital volume are both strongly associated with mortality. These findings suggest that open surgery should be concentrated in hospitals and surgeons with high volume.
Copyright © 2016 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Invited commentary.J Vasc Surg. 2017 Mar;65(3):634. doi: 10.1016/j.jvs.2016.10.003. J Vasc Surg. 2017. PMID: 28236915 No abstract available.
References
-
- Dimick JB, Cowan JA, Jr, Stanley JC, Henke PK, Pronovost PJ, Upchurch GR., Jr Surgeon specialty and provider volumes are related to outcome of intact abdominal aortic aneurysm repair in the United States. J Vasc Surg. 2003;38(4):739–44. - PubMed
-
- McPhee JT, Robinson WP, 3rd, Eslami MH, Arous EJ, Messina LM, Schanzer A. Surgeon case volume, not institution case volume, is the primary determinant of in-hospital mortality after elective open abdominal aortic aneurysm repair. J Vasc Surg. 2011;53(3):591–9. e2. - PubMed
-
- Holt PJ, Poloniecki JD, Gerrard D, Loftus IM, Thompson MM. Meta-analysis and systematic review of the relationship between volume and outcome in abdominal aortic aneurysm surgery. Br J Surg. 2007;94(4):395–403. - PubMed
-
- Birkmeyer JD, Stukel TA, Siewers AE, Goodney PP, Wennberg DE, Lucas FL. Surgeon volume and operative mortality in the United States. N Engl J Med. 2003;349(22):2117–27. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
