

Talimogene Laherparepvec (T-VEC) and Other Oncolytic Viruses for the Treatment of Melanoma
- PMID: 27988837
- PMCID: PMC8977104
- DOI: 10.1007/s40257-016-0238-9
Talimogene Laherparepvec (T-VEC) and Other Oncolytic Viruses for the Treatment of Melanoma
Abstract
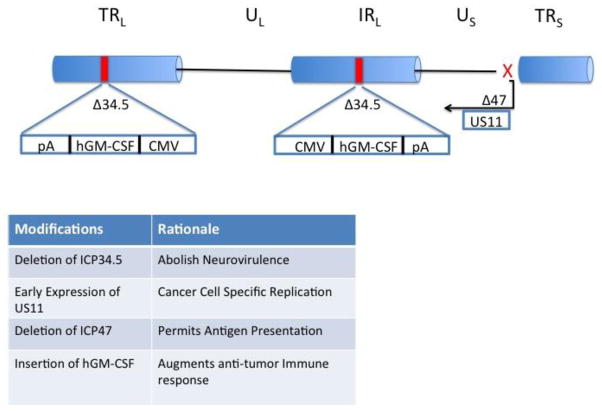
Many mammalian viruses have properties that can be commandeered for the treatment of cancer. These characteristics include preferential infection and replication in tumor cells, the initiation of tumor cell lysis, and the induction of innate and adaptive anti-tumor immunity. Furthermore, viruses can be genetically engineered to reduce pathogenicity and increase immunogenicity resulting in minimally toxic therapeutic agents. Talimogene laherparepvec (T-VEC; Imlygic™), is a genetically modified herpes simplex virus, type 1, and is the first oncolytic virus therapy to be approved for the treatment of advanced melanoma by the US FDA. T-VEC is attenuated by the deletion of the herpes neurovirulence viral genes and enhanced for immunogenicity by the deletion of the viral ICP47 gene. Immunogenicity is further supported by expression of the human granulocyte-macrophage colony-stimulating factor (GM-CSF) gene, which helps promote the priming of T cell responses. T-VEC demonstrated significant improvement in durable response rate, objective response rate, and progression-free survival in a randomized phase III clinical trial for patients with advanced melanoma. This review will discuss the optimal selection of patients for such treatment and describe how therapy is optimally delivered. We will also discuss future directions for oncolytic virus immunotherapy, which will likely include combination T-VEC clinical trials, expansion of T-VEC to other types of non-melanoma skin cancers, and renewed efforts at oncolytic virus drug development with other viruses.
Conflict of interest statement
Dr. Kaufman has served on advisory boards for Amgen, Celldex, EMD Serono, Merck, Prometheus and Sanofi. He is a member of the Merck Speaker’s Bureau but does not received direct compensation for this activity. Mr. Bommareddy, Dr. Patel and Dr. Hossain have no conflicts to declare.
Figures
References
-
- Brunssen A, et al. Impact of skin cancer screening and secondary prevention campaigns on skin cancer incidence and mortality: A systematic review. J Am Acad Dermatol. 2016 - PubMed
-
- Feng Z, Zhang Z, Wu XC. Lifetime risks of cutaneous melanoma by histological subtype and race/ethnicity in the United States. J La State Med Soc. 2013;165(4):201–8. - PubMed
-
- Coit DG, et al. NCCN Guidelines Insights: Melanoma, Version 3.2016. J Natl Compr Canc Netw. 2016;14(8):945–58. - PubMed
-
- Lau PK, Ascierto PA, McArthur G. Melanoma: the intersection of molecular targeted therapy and immune checkpoint inhibition. Curr Opin Immunol. 2016;39:30–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
