

Robotic surgery in gynecology
- PMID: 27990092
- PMCID: PMC5147762
- DOI: 10.5152/jtgga.2016.16187
Robotic surgery in gynecology
Abstract
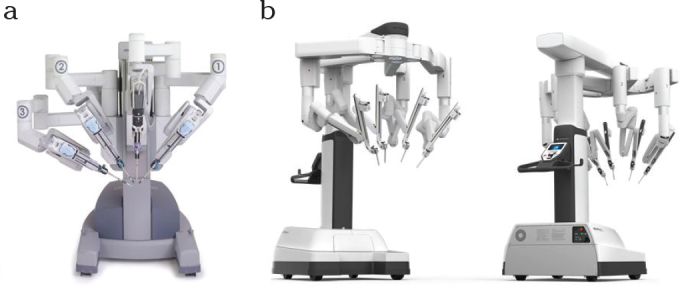
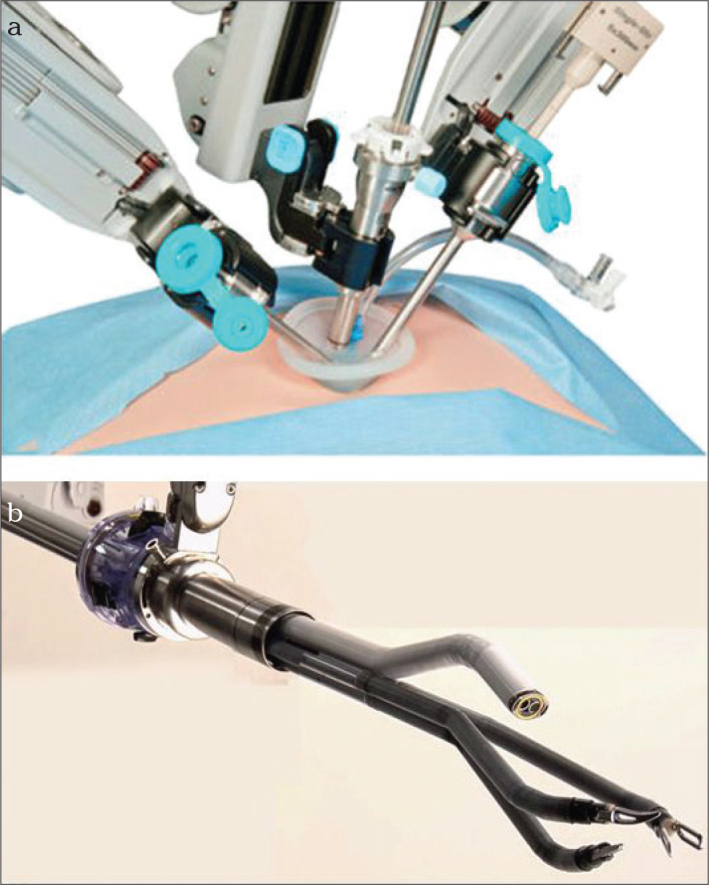
Robotic surgery is the most dynamic development in the sector of minimally invasive operations currently. It should not be viewed as an alternative to laparoscopy, but as the next step in a process of technological evolution. The advancement of robotic surgery, in terms of the introduction of the Da Vinci Xi, permits the variable use of optical devices in all four trocars. Due to the new geometry of the "patient cart," an operation can be performed in all spatial directions without re-docking. Longer instruments and the markedly narrower mechanical elements of the "patient cart" provide greater flexibility as well as access similar to those of traditional laparoscopy. Currently, robotic surgery is used for a variety of indications in the treatment of benign gynecological diseases as well as malignant ones. Interdisciplinary cooperation and cooperation over large geographical distances have been rendered possible by telemedicine, and will ensure comprehensive patient care in the future by highly specialized surgery teams. In addition, the second operation console and the operation simulator constitute a new dimension in advanced surgical training. The disadvantages of robotic surgery remain the high costs of acquisition and maintenance as well as the laborious training of medical personnel before they are confident with using the technology.
Keywords: Robotic surgery; cost efficiency; gynecological oncology; laparoscopy; surgical training.
Conflict of interest statement
No conflict of interest was declared by the authors.
Figures
References
-
- Liu H, Lu D, Wang L, Shi G, Song H, Clarke J. Robotic surgery for benign gynaecological disease. Cochrane Database Syst Rev. 2012;2:CD008978. https://doi.org/10.1002/14651858.cd008978.pub2. - DOI - PubMed
-
- Schollmeyer T, Mettler L, Alkatout I. Roboterchirurgie in der Gynäkologie - Der Operateur am Schreibtisch. Der Gynäkologe. 2011:196–201. https://doi.org/10.1007/s00129-010-2709-z. - DOI
-
- Yuh B, Yu X, Raytis J, Lew M, Fong Y, Lau C. Use of a mobile tower-based robot--The initial Xi robot experience in surgical oncology. J Surg Oncol. 2016;113:5–7. https://doi.org/10.1002/jso.24094. - DOI - PubMed
-
- Sinha R, Sanjay M, Rupa B, Kumari S. Robotic surgery in gynecology. J Minim Access Surg. 2015;11:50–9. https://doi.org/10.4103/0972-9941.147690. - DOI - PMC - PubMed
-
- Herron DM, Marohn M SAGES-MIRA Robotic Surgery Consensus Group. A consensus document on robotic surgery. Surg Endosc. 2008;22:313–25. discussion 311–2. https://doi.org/10.1007/s00464-007-9727-5. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources