

Combined Acute Haemolytic and Secondary Angle Closure Glaucoma following Spontaneous Intraocular Haemorrhages in a Patient on Warfarin
- PMID: 27990116
- PMCID: PMC5155631
- DOI: 10.1159/000452440
Combined Acute Haemolytic and Secondary Angle Closure Glaucoma following Spontaneous Intraocular Haemorrhages in a Patient on Warfarin
Abstract
Background: To report the first described case of combined haemolytic and acute angle closure glaucoma secondary to spontaneous intraocular haemorrhages in a patient on excessive anticoagulation. To the best of our knowledge, this is the first case reported in the literature presenting with raised intraocular pressure due to both mechanisms.
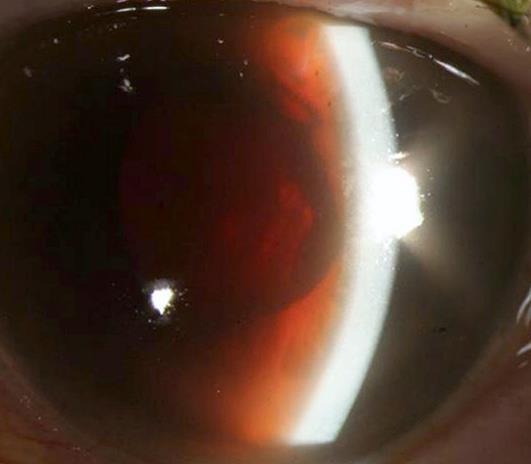
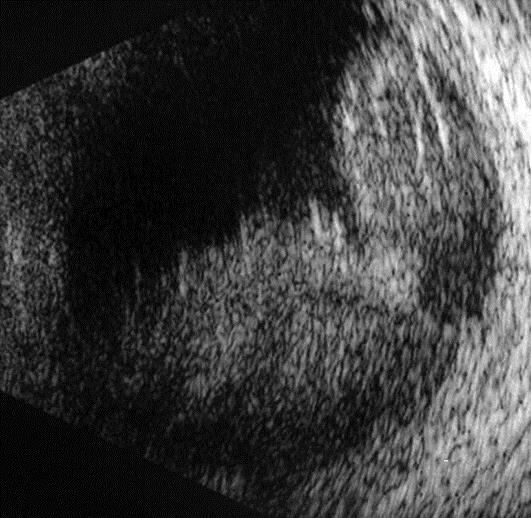
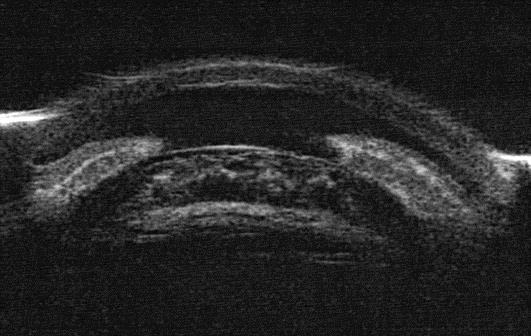
Case description: A 90-year-old woman presented with acute pain and reduction in vision in the left eye. Her intraocular pressure (IOP) was 55 mm Hg. There were red tinted blood cells in the anterior chamber giving it a reddish hue. The patient was known to have advanced wet macular degeneration. She was taking oral warfarin for atrial fibrillation. Her international normalised ratio (INR) was 7.7. B-scan ultrasound of posterior segment showed vitreous and suprachoroidal haemorrhages. An ultrabiomicroscopic examination confirmed open angles. A diagnosis of haemolytic glaucoma secondary to intraocular haemorrhages was made. The IOP was controlled medically. Warfarin was withdrawn and oral vitamin K therapy was initiated leading to a rapid INR reduction. Three days later, her anterior chamber became progressively shallower causing a secondary acute angle closure which was managed medically. After 2 months, the left IOP was well-controlled without any medications and the eye was not inflamed. Her vision in that eye remained perception of light.
Conclusion: Patients with suprachoroidal haemorrhages should be closely monitored as they might subsequently develop acute angle closure despite an initially open angle and well-controlled INR and IOP. Excessive anticoagulation needs to be prevented to minimise the risk of sight-threatening complications.
Keywords: Angle closure; Anticoagulants; Haemolytic glaucoma; Macular degeneration; Suprachoroidal haemorrhage.
Figures
Similar articles
-
A rare case of acute angle closure due to spontaneous suprachoroidal haemorrhage secondary to loss of anti-coagulation control: a case report.BMC Ophthalmol. 2018 Sep 14;18(Suppl 1):224. doi: 10.1186/s12886-018-0857-4. BMC Ophthalmol. 2018. PMID: 30255796 Free PMC article.
-
Hidden Kiss: A Rare Case of Spontaneous Suprachoroidal Hemorrhage Masquerading as Vitreous Hemorrhage Causing Secondary Angle-Closure Glaucoma.Cureus. 2023 Aug 1;15(8):e42817. doi: 10.7759/cureus.42817. eCollection 2023 Aug. Cureus. 2023. PMID: 37664398 Free PMC article.
-
Spontaneous suprachoroidal and orbital hemorrhage in an older woman associated with prophylactic antiplatelet therapy: A case report and literature review.Heliyon. 2022 Nov 11;8(11):e11511. doi: 10.1016/j.heliyon.2022.e11511. eCollection 2022 Nov. Heliyon. 2022. PMID: 36411881 Free PMC article.
-
Acute angle closure glaucoma.Br J Hosp Med (Lond). 2019 Dec 2;80(12):C174-C179. doi: 10.12968/hmed.2019.80.12.C174. Br J Hosp Med (Lond). 2019. PMID: 31822188 Review.
-
The effect of cataract extraction on intraocular pressure.Curr Opin Ophthalmol. 2010 Mar;21(2):118-22. doi: 10.1097/ICU.0b013e3283360ac3. Curr Opin Ophthalmol. 2010. PMID: 20040874 Review.
Cited by
-
Massive Spontaneous Suprachoroidal Hemorrhage in a Patient With Type 1 Chronic Myeloid Leukemia and Lymphoplasmacytic Lymphoma: Case Report and Review of the Literature.J Vitreoretin Dis. 2022 May 25;6(3):214-220. doi: 10.1177/24741264221074799. eCollection 2022 May-Jun. J Vitreoretin Dis. 2022. PMID: 37008555 Free PMC article. Review.
-
Vitamin K and the Visual System-A Narrative Review.Nutrients. 2023 Apr 18;15(8):1948. doi: 10.3390/nu15081948. Nutrients. 2023. PMID: 37111170 Free PMC article. Review.
-
Spontaneous suprachoroidal hemorrhage in a high myopia patient with rhegmatogenous retinal detachment: a case report and literature review.Biosci Rep. 2019 Jun 25;39(6):BSR20181454. doi: 10.1042/BSR20181454. Print 2019 Jun 28. Biosci Rep. 2019. PMID: 31160485 Free PMC article.
References
-
- Phelps CD, Watzke RC. Hemolytic glaucoma. Am J Ophthalmol. 1975;80:690–695. - PubMed
-
- Singh H, Grand MG. Treatment of blood-induced glaucoma by trans pars plana vitrectomy. Retina. 1981;1:255–257. - PubMed
-
- Chu TG, Green RL. Suprachoroidal hemorrhage. Surv Ophthalmol. 1999;43:471–486. - PubMed
-
- Knox FA, Johnston PB. Spontaneous suprachoroidal haemorrhage in a patient with age-related macular degeneration on excessive anticoagulation therapy. Eye. 2002;16:669–670. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
