

Standards and Guidelines for the Interpretation and Reporting of Sequence Variants in Cancer: A Joint Consensus Recommendation of the Association for Molecular Pathology, American Society of Clinical Oncology, and College of American Pathologists
- PMID: 27993330
- PMCID: PMC5707196
- DOI: 10.1016/j.jmoldx.2016.10.002
Standards and Guidelines for the Interpretation and Reporting of Sequence Variants in Cancer: A Joint Consensus Recommendation of the Association for Molecular Pathology, American Society of Clinical Oncology, and College of American Pathologists
Abstract
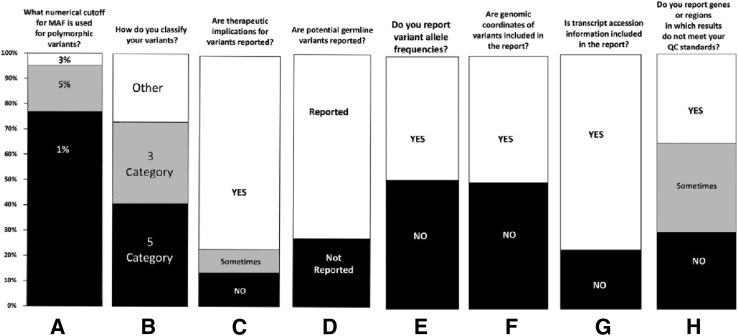
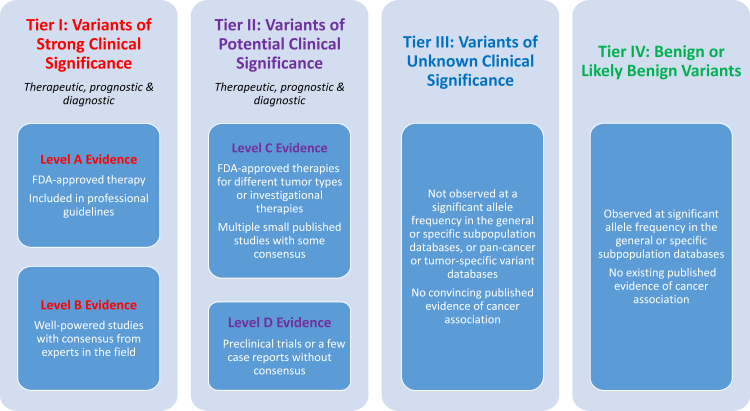
Widespread clinical laboratory implementation of next-generation sequencing-based cancer testing has highlighted the importance and potential benefits of standardizing the interpretation and reporting of molecular results among laboratories. A multidisciplinary working group tasked to assess the current status of next-generation sequencing-based cancer testing and establish standardized consensus classification, annotation, interpretation, and reporting conventions for somatic sequence variants was convened by the Association for Molecular Pathology with liaison representation from the American College of Medical Genetics and Genomics, American Society of Clinical Oncology, and College of American Pathologists. On the basis of the results of professional surveys, literature review, and the Working Group's subject matter expert consensus, a four-tiered system to categorize somatic sequence variations based on their clinical significances is proposed: tier I, variants with strong clinical significance; tier II, variants with potential clinical significance; tier III, variants of unknown clinical significance; and tier IV, variants deemed benign or likely benign. Cancer genomics is a rapidly evolving field; therefore, the clinical significance of any variant in therapy, diagnosis, or prognosis should be reevaluated on an ongoing basis. Reporting of genomic variants should follow standard nomenclature, with testing method and limitations clearly described. Clinical recommendations should be concise and correlate with histological and clinical findings.
Copyright © 2017 American Society for Investigative Pathology and the Association for Molecular Pathology. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Identification of Germline Variants in Tumor Genomic Sequencing Analysis.J Mol Diagn. 2018 Jan;20(1):123-125. doi: 10.1016/j.jmoldx.2017.09.008. J Mol Diagn. 2018. PMID: 29249243
-
Authors' Reply.J Mol Diagn. 2018 Jan;20(1):125-126. doi: 10.1016/j.jmoldx.2017.11.002. J Mol Diagn. 2018. PMID: 29249244 Free PMC article.
References
-
- Garraway L.A., Verweij J., Ballman K.V. Precision oncology: an overview. J Clin Oncol. 2013;31:1803–1805. - PubMed
-
- Von Hoff D.D., Stephenson J.J., Rosen P., Loesch D.M., Borad M.J., Anthony S., Jameson G., Brown S., Cantafio N., Richards D.A., Fitch T.R., Wasserman E., Fernandez C., Green S., Sutherland W., Bittner M., Alarcon A., Mallery D., Penny R. Pilot study using molecular profiling of patients' tumors to find potential targets and select treatments for their refractory cancers. J Clin Oncol. 2010;28:4877–4883. - PubMed
-
- Tsimberidou A.-M., Iskander N.G., Hong D.S., Wheler J.J., Falchook G.S., Fu S., Piha-Paul S., Naing A., Janku F., Luthra R., Ye Y., Wen S., Berry D., Kurzrock R. Personalized medicine in a phase I clinical trials program: the MD Anderson Cancer Center initiative. Clin Cancer Res. 2012;18:6373–6383. - PMC - PubMed
-
- Shendure J., Ji H. Next-generation DNA sequencing. Nat Biotechnol. 2008;26:1135–1145. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
