

Increased Costs Associated with Bloodstream Infections Caused by Multidrug-Resistant Gram-Negative Bacteria Are Due Primarily to Patients with Hospital-Acquired Infections
- PMID: 27993852
- PMCID: PMC5328522
- DOI: 10.1128/AAC.01709-16
Increased Costs Associated with Bloodstream Infections Caused by Multidrug-Resistant Gram-Negative Bacteria Are Due Primarily to Patients with Hospital-Acquired Infections
Abstract
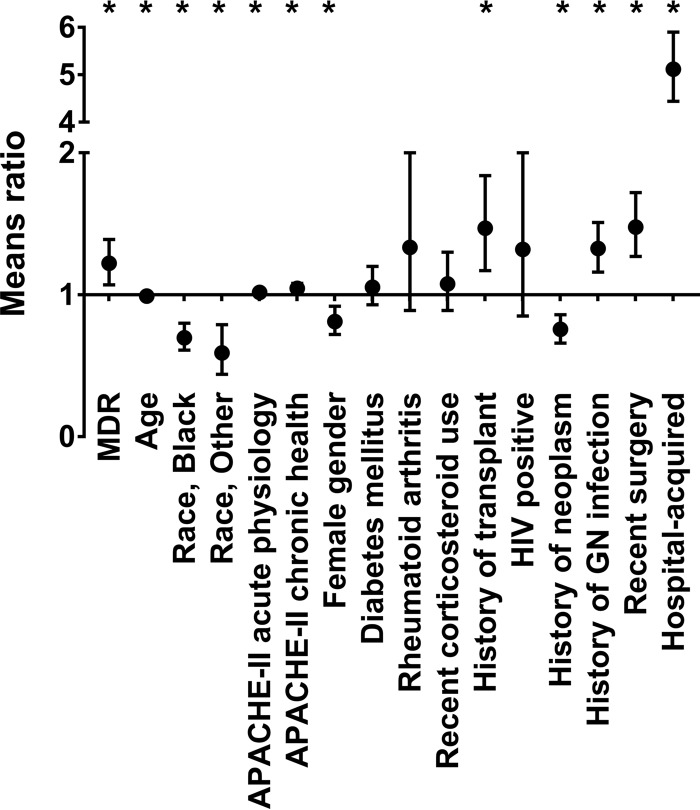
The clinical and economic impacts of bloodstream infections (BSI) due to multidrug-resistant (MDR) Gram-negative bacteria are incompletely understood. From 2009 to 2015, all adult inpatients with Gram-negative BSI at our institution were prospectively enrolled. MDR status was defined as resistance to ≥3 antibiotic classes. Clinical outcomes and inpatient costs associated with the MDR phenotype were identified. Among 891 unique patients with Gram-negative BSI, 292 (33%) were infected with MDR bacteria. In an adjusted analysis, only history of Gram-negative infection was associated with MDR BSI versus non-MDR BSI (odds ratio, 1.60; 95% confidence interval [CI], 1.19 to 2.16; P = 0.002). Patients with MDR BSI had increased BSI recurrence (1.7% [5/292] versus 0.2% [1/599]; P = 0.02) and longer hospital stay (median, 10.0 versus 8.0 days; P = 0.0005). Unadjusted rates of in-hospital mortality did not significantly differ between MDR (26.4% [77/292]) and non-MDR (21.7% [130/599]) groups (P = 0.12). Unadjusted mean costs were 1.62 times higher in MDR than in non-MDR BSI ($59,266 versus $36,452; P = 0.003). This finding persisted after adjustment for patient factors and appropriate empirical antibiotic therapy (means ratio, 1.18; 95% CI, 1.03 to 1.36; P = 0.01). Adjusted analysis of patient subpopulations revealed that the increased cost of MDR BSI occurred primarily among patients with hospital-acquired infections (MDR means ratio, 1.41; 95% CI, 1.10 to 1.82; P = 0.008). MDR Gram-negative BSI are associated with recurrent BSI, longer hospital stays, and increased mean inpatient costs. MDR BSI in patients with hospital-acquired infections primarily account for the increased cost.
Keywords: Gram negative; bloodstream infection; cost.
Copyright © 2017 American Society for Microbiology.
Figures
References
-
- The Review on Antimicrobial Resistance. 11 December 2014, posting date. Antimicrobial resistance: tackling a crisis for the future health and wealth of nations. https://amr-review.org/sites/default/files/AMR Accessed 3 June 2016.
-
- Magiorakos AP, Srinivasan A, Carey RB, Carmeli Y, Falagas ME, Giske CG, Harbarth S, Hindler JF, Kahlmeter G, Olsson-Liljequist B, Paterson DL, Rice LB, Stelling J, Struelens MJ, Vatopoulos A, Weber JT, Monnet DL. 2012. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect 18:268–281. doi: 10.1111/j.1469-0691.2011.03570.x. - DOI - PubMed
-
- Apisarnthanarak A, Kiratisin P, Saifon P, Kitphati R, Dejsirilert S, Mundy LM. 2007. Clinical and molecular epidemiology of community-onset, extended-spectrum beta-lactamase-producing Escherichia coli infections in Thailand: a case-case-control study. Am J Infect Control 35:606–612. doi: 10.1016/j.ajic.2007.05.008. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
