

Streptococcus agalactiae Endophthalmitis in Boston Keratoprosthesis in a Patient with Steven-Johnson Syndrome
- PMID: 27994401
- PMCID: PMC5141631
- DOI: 10.4103/0974-9233.194095
Streptococcus agalactiae Endophthalmitis in Boston Keratoprosthesis in a Patient with Steven-Johnson Syndrome
Abstract
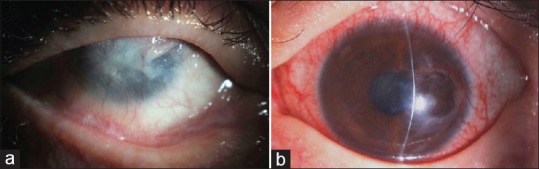
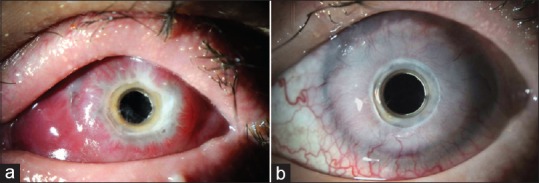
A 25-year-old Syrian male with a previous episode of Stevens-Johnson syndrome with bilateral corneal cicatrization previously underwent surgery for Type 1 Boston Keratoprosthesis (K-Pro). Sixteen months after the K-Pro surgery, the patient presented with decreased vision to hand motion and microbial keratitis of the graft around the K-Pro with purulent discharge. Corneal scrapings were nonrevealing. B-scan in 3 days showed increased debris in the vitreous cavity and thickened retinochoroidal layer. Intravitreal tap and injections of vancomycin and ceftazidime were performed. The vitreous culture revealed β-hemolytic Streptococcus agalactiae; fungal cultures were negative. Repeat B-scan 3 days later demonstrated decreased vitreous opacity, and the patient felt more comfortable and was without pain. His visual acuity improved to 20/70, ocular findings have been stable for 9 months, and the patient continues to be monitored.
Keywords: Boston Keratoprosthesis; Endophthalmitis; Steven–Johnson Syndrome; Streptococcus agalactiae.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Netland PA, Terada H, Dohlman CH. Glaucoma associated with keratoprosthesis. Ophthalmology. 1998;105:751–7. - PubMed
-
- Yaghouti F, Nouri M, Abad JC, Power WJ, Doane MG, Dohlman CH. Keratoprosthesis: Preoperative prognostic categories. Cornea. 2001;20:19–23. - PubMed
-
- Dohlman CH, Abad JC, Dudenhoefer EJ. Keratoprosthesis: Beyond corneal graft failure. In: Spaeth G, editor. Ophthalmic Surgery-Principles and Practice. 3rd ed. Philadelphia, PA: WB Sanders; 2002. pp. 199–207.
-
- Ray S, Khan BF, Dohlman CH, D’Amico DJ. Management of vitreoretinal complications in eyes with permanent keratoprosthesis. Arch Ophthalmol. 2002;120:559–66. - PubMed
-
- Dohlman CH, Barnes SD, Ma JK. Keratoprosthesis. In: Krachmer JH, Mannis MJ, Holland EJ, editors. Cornea. 2nd ed. Edinburgh: Elsevier; 2005. pp. 1719–28.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
