

Peculiarities in Ankle Cartilage
- PMID: 27994716
- PMCID: PMC5154419
- DOI: 10.1177/1947603516642572
Peculiarities in Ankle Cartilage
Abstract
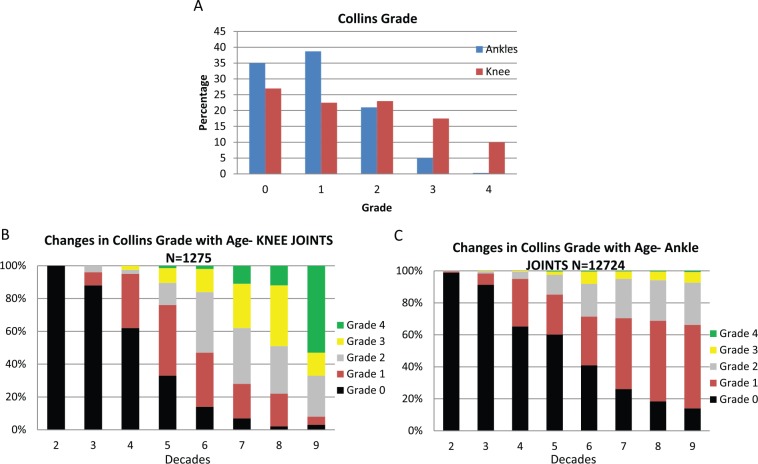
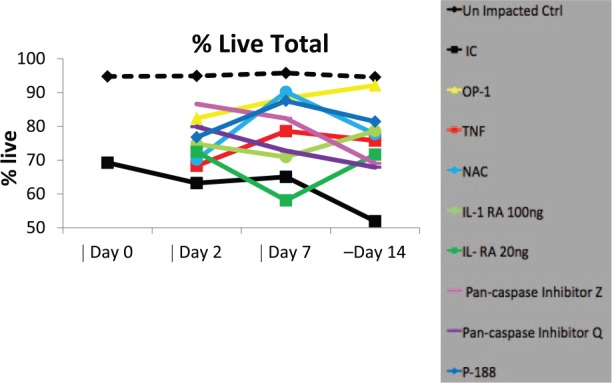
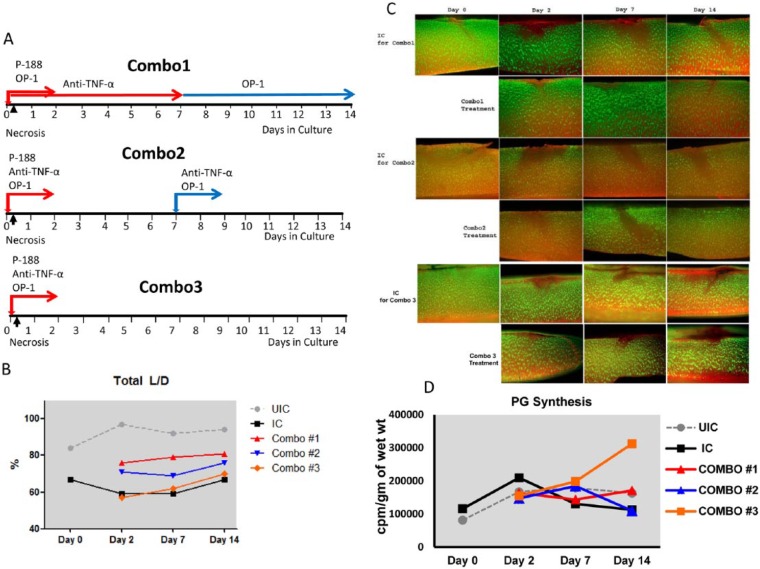
Posttraumatic osteoarthritis (PTOA) is the most common form of osteoarthritis (OA) of the ankle joint. PTOA occurs as a result of several factors, including the poor regenerative capacity of hyaline articular cartilage as well as increased contact stresses following trauma. The purpose of this article is to review the epidemiology, pathogenesis, and potential targets for treatment of PTOA in the ankle joint. Previous reviews primarily addressed clinical approaches to ankle PTOA, while the focus of the current article will be specifically on the newly acquired knowledge of the cellular mechanisms that drive PTOA in the ankle joint and means for potential targeted therapeutics that might halt the progression of cartilage degeneration and/or improve the outcome of surgical interventions. Three experimental treatment strategies are discussed in this review: (1) increasing the anabolic potential of chondrocytes through treatment with growth factors such as bone morphogenetic protein-7; (2) limiting chondrocyte cell death either through the protection of cell membrane with poloxamer 188 or inhibiting activity of intracellular proteases, caspases, which are responsible for cell death by apoptosis; and (3) inhibiting catabolic/inflammatory responses of chondrocytes by treating them with anti-inflammatory agents such as tumor necrosis factor-α antagonists. Future studies should focus on identifying the appropriate timing for treatment and an appropriate combination of anti-inflammatory, chondro- and matrix-protective biologics to limit the progression of trauma-induced cartilage degeneration and prevent the development of PTOA in the ankle joint.
Keywords: ankle; anti-inflammatory; cartilage; chondroprotection; posttraumatic osteoarthritis.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Huch K, Kuettner KE, Dieppe P. Osteoarthritis in ankle and knee joints. Semin Arthritis Rheum. 1997;26(4):667-74. - PubMed
-
- Brown TD, Johnston RC, Saltzman CL, Marsh JL, Buckwalter JA. Posttraumatic osteoarthritis: a first estimate of incidence, prevalence, and burden of disease. J Orthop Trauma. 2006;20(10):739-44. - PubMed
-
- Polyzois VD, Papakostas I, Zgonis T, Polyzois DG, Soucacos PN. Current concepts and techniques in posttraumatic arthritis. Clin Podiatr Med Surg. 2006;23(2):455-65. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
