

Current Technical Issues for Surgery of Primary Liver Cancer
- PMID: 27995088
- PMCID: PMC5159717
- DOI: 10.1159/000449345
Current Technical Issues for Surgery of Primary Liver Cancer
Abstract
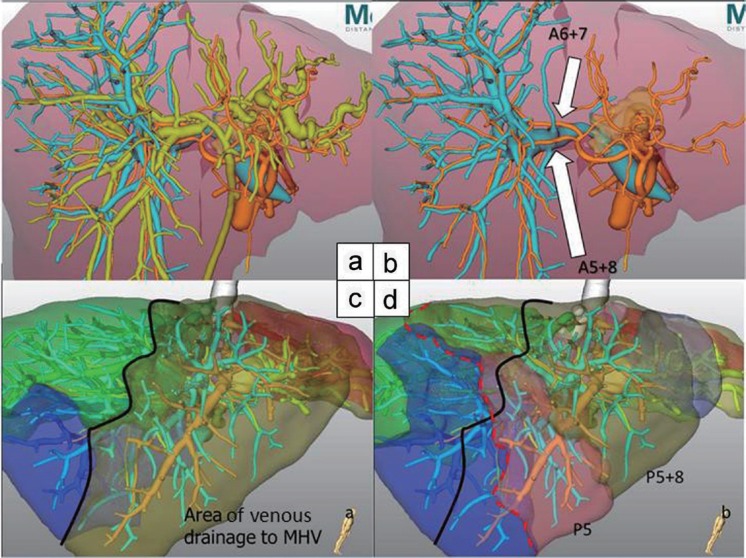
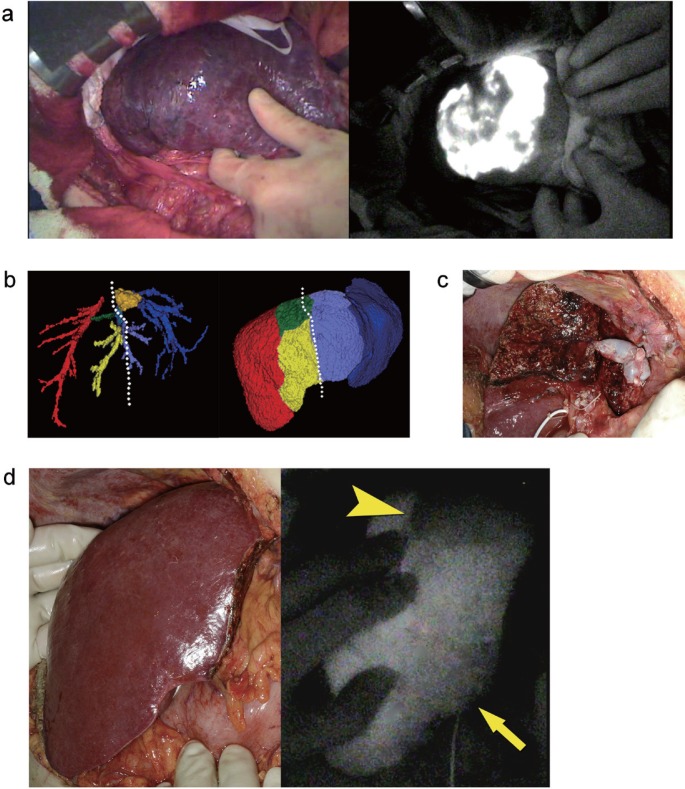
Primary liver cancer is the fifth most common cancer worldwide. Apart from liver transplantation, surgical resection has been accepted as the effective local treatment for hepatocellular carcinoma (HCC), one of the most common primary liver cancers. Recent technological innovations including navigation technology and intraoperative real-time fluorescence guidance have been utilized for liver resections in clinical practice. With respect to liver resection techniques, the laparoscopic approach has been increasingly gaining popularity as one of the minimally-invasive treatments of HCC. These technological innovations and technical advancements are expected to further improve the safety and efficacy of liver resections.
Keywords: Fluorescence imaging technique; Hepatocellular carcinoma; Intrahepatic cholangiocellular carcinoma; Laparoscopic liver resection; Three-dimensional computed tomography.
Figures
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Imamura H, Seyama Y, Kokudo N, Maema A, Sugawara Y, Sano K, Takayama T, Makuuchi M. One thousand fifty-six hepatectomies without mortality in 8 years. Arch Surg. 2003;138:1198–1206. discussion 1206. - PubMed
-
- Wakabayashi G, Cherqui D, Geller DA, et al. Recommendations for laparoscopic liver resection: a report from the second international consensus conference held in Morioka. Ann Surg. 2015;261:619–629. - PubMed
-
- Endo I, House MG, Klimstra DS, Gönen M, D'Angelica M, Dematteo RP, Fong Y, Blumgart LH, Jarnagin WR. Clinical significance of intraoperative bile duct margin assessment for hilar cholangiocarcinoma. Ann Surg Oncol. 2008;15:2104–2112. - PubMed
-
- Kenjo A, Miyata H, Gotoh M, Kitagawa Y, Shimada M, Baba H, Tomita N, Kimura W, Sugihara K, Mori M. Risk stratification of 7,732 hepatectomy cases in 2011 from the National Clinical Database for Japan. J Am Coll Surg. 2014;218:412–422. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
