

A systematic and technical guide on how to reduce a shoulder dislocation
- PMID: 27995208
- PMCID: PMC5154590
- DOI: 10.1016/j.tjem.2016.09.008
A systematic and technical guide on how to reduce a shoulder dislocation
Abstract
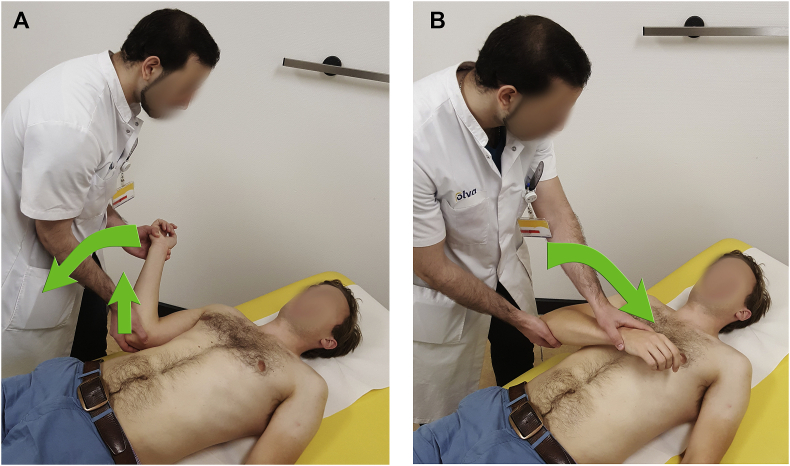
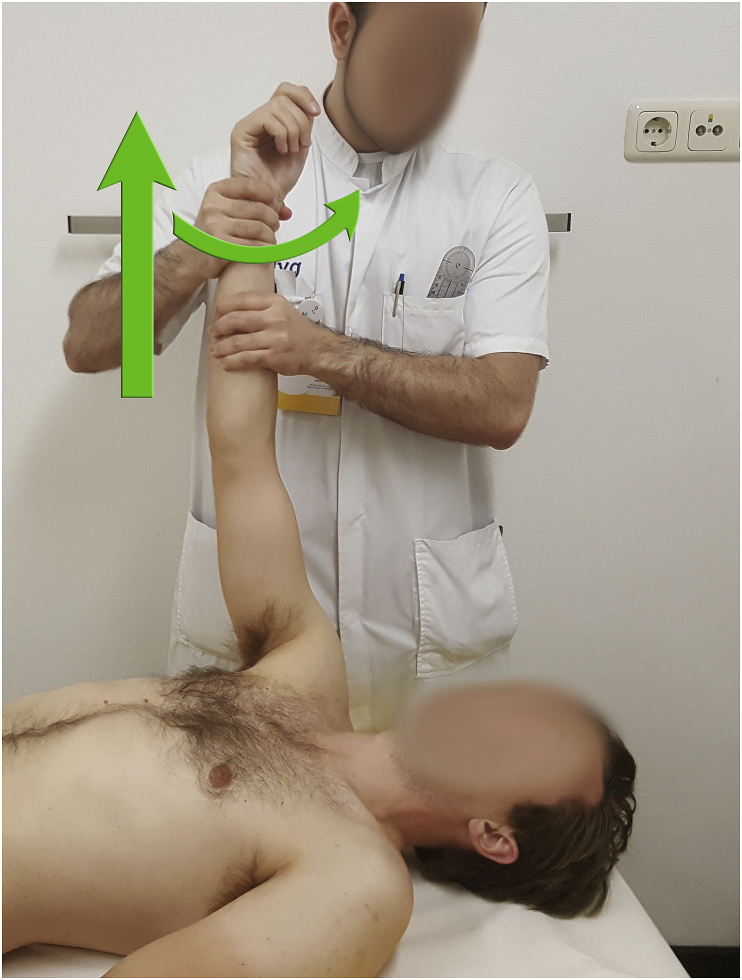
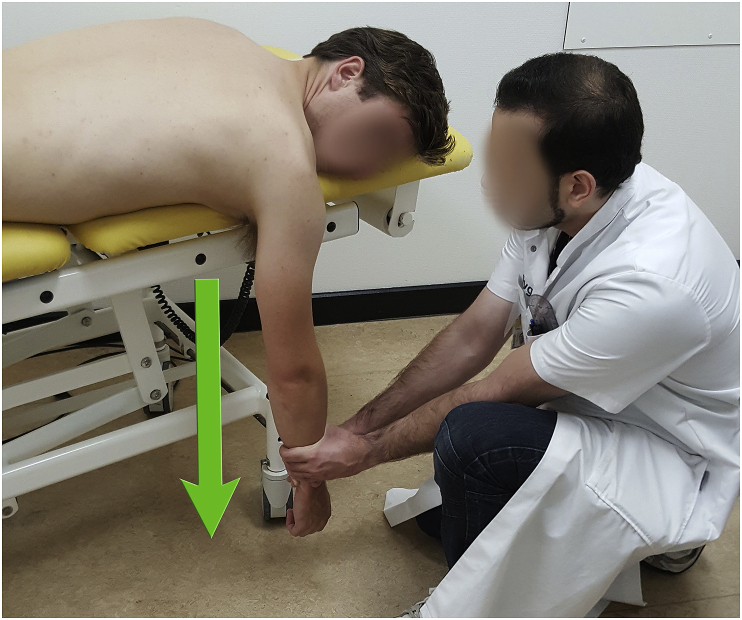
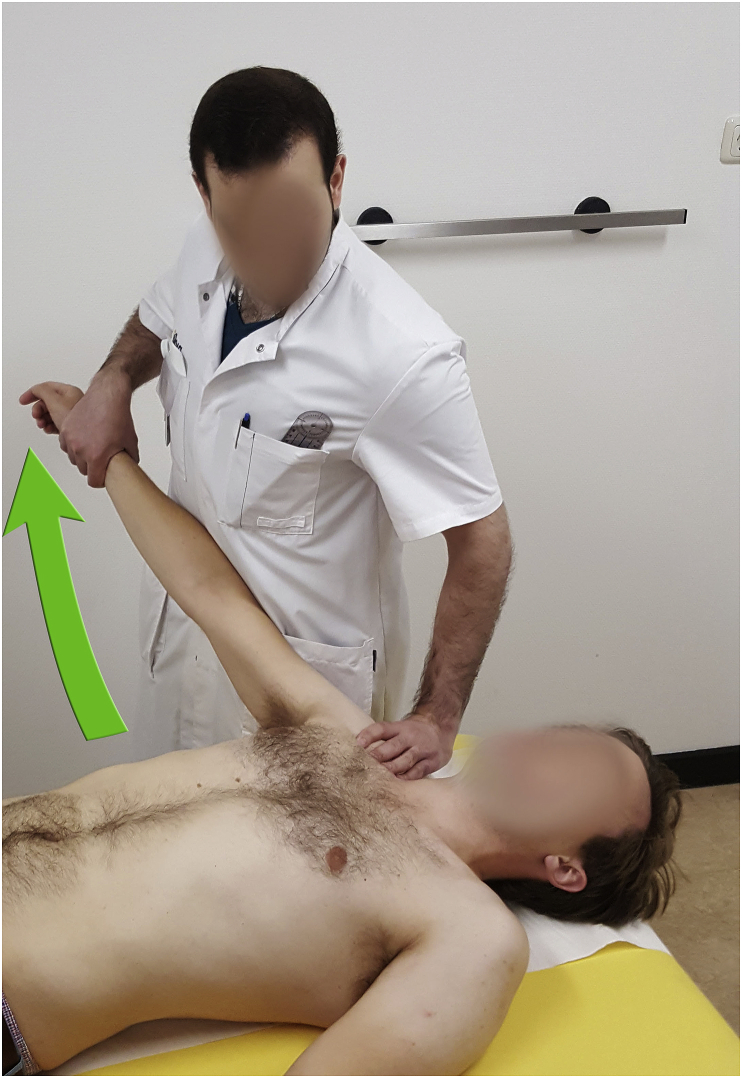
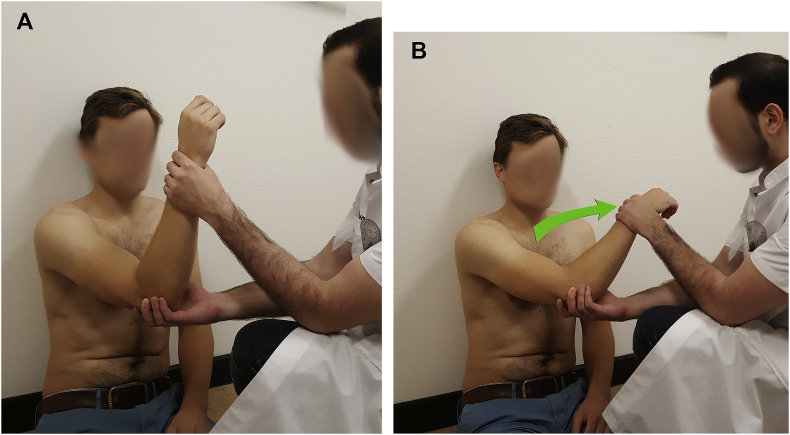
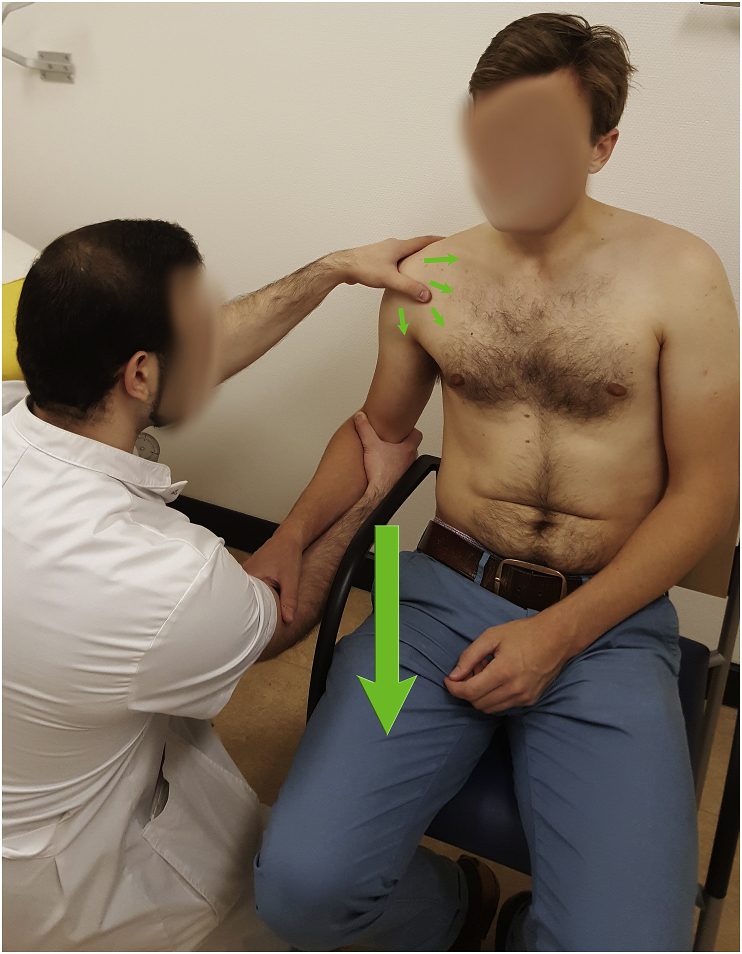
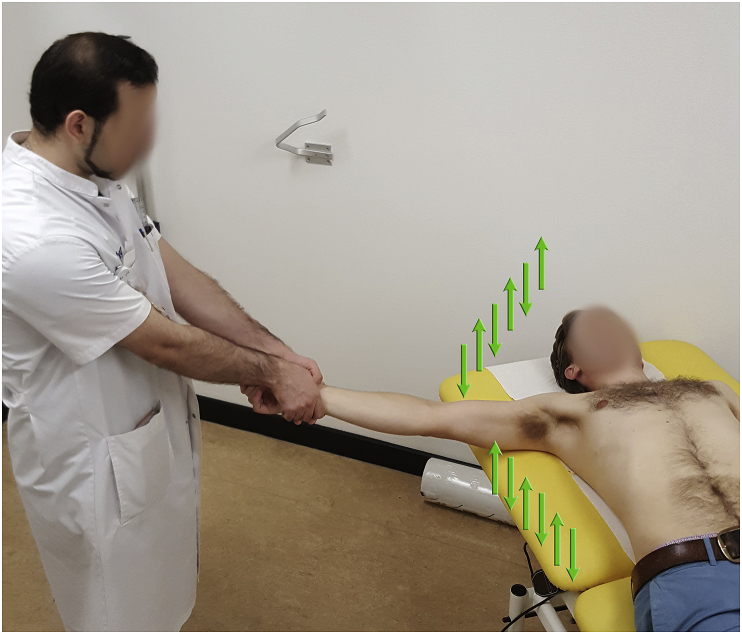
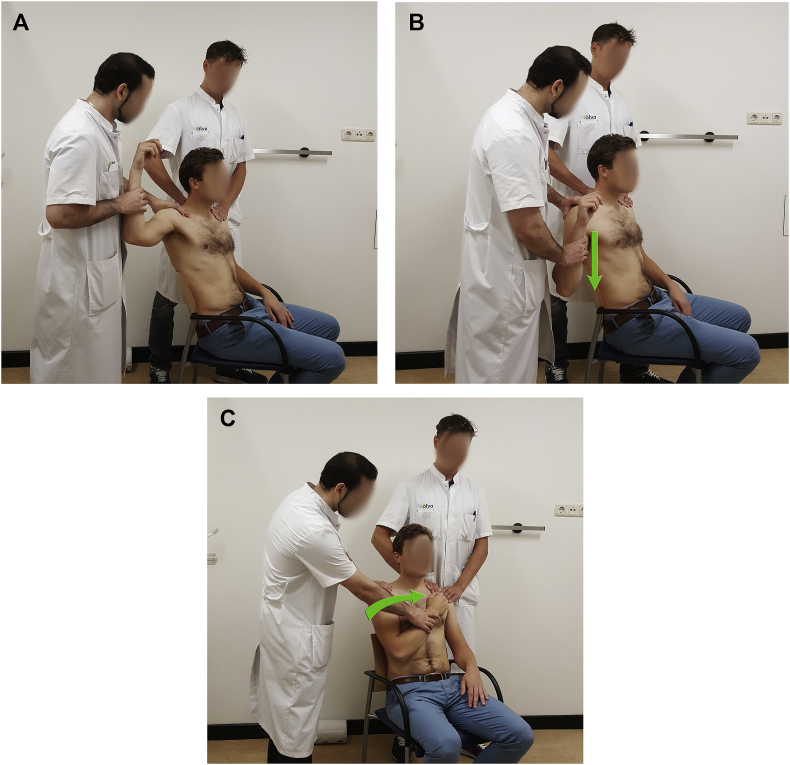
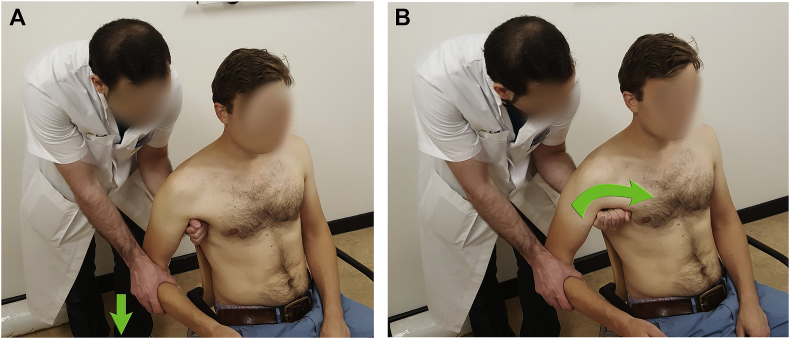
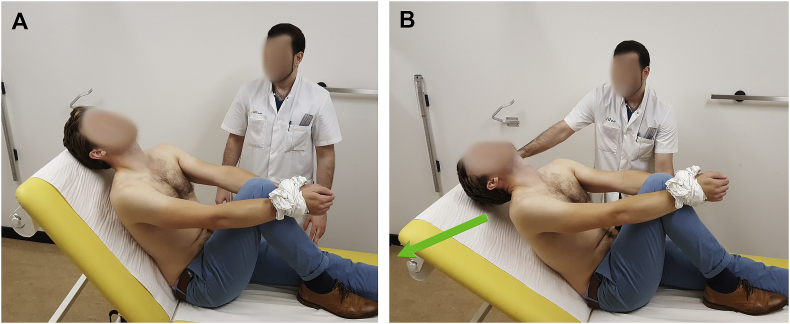
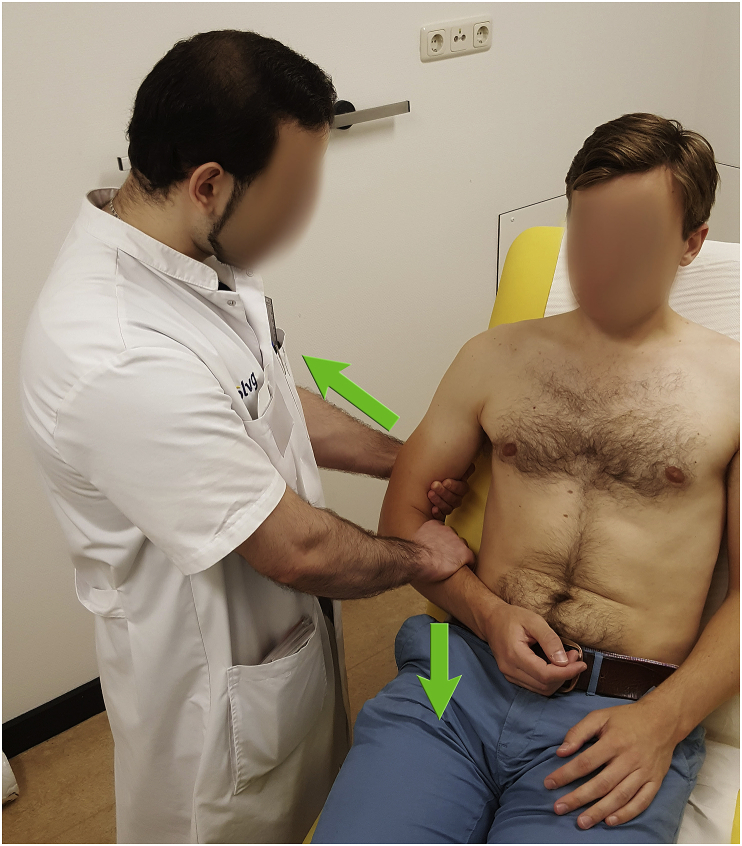
Objectives: Our objective is to provide a systematic and technical guide on how to reduce a shoulder dislocation, based on techniques that have been described in literature for patients with anterior and posterior shoulder instability.
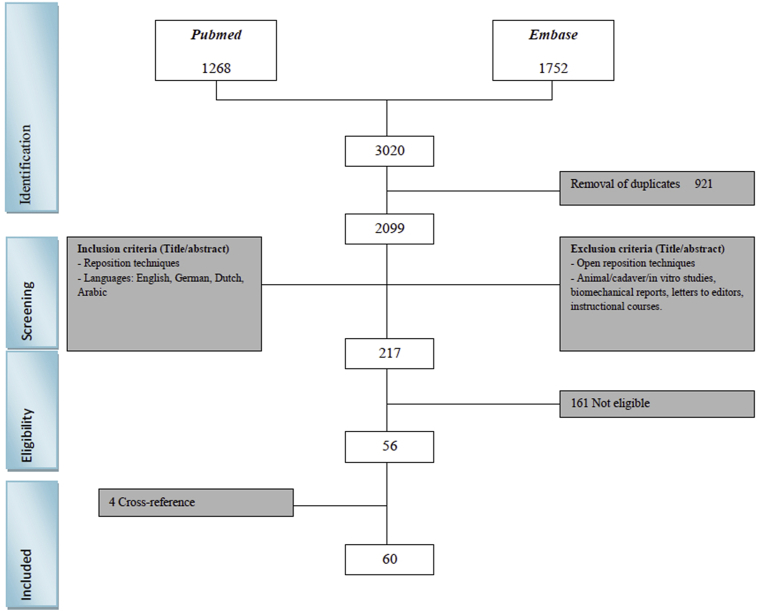
Materials and methods: A PubMed and EMBASE query was performed, screening all relevant literature on the closed reduction techniques. Studies regarding open reduction techniques and studies with fracture dislocations were excluded.
Results: In this study we give an overview of 23 different techniques for closed reduction and 17 modifications of these techniques.
Discussion: In this review article we present a complete overview of the techniques, that have been described in the literature for closed reduction for shoulder dislocations. This manuscript can be regarded as a clinical guide how to perform a closed reduction maneuver, including several technical tips and tricks to optimize the success rate and to avoid complications.
Conclusion: There are 23 different reduction techniques with 17 modifications of these techniques. Knowledge of the different techniques is highly important for a good reduction.
Keywords: Glenohumeral; Instability; Maneuver; Reposition; Shoulder; Techniques.
Figures











References
-
- Schaider J.S.R. Clinical Practice of Emergency Medicine. Philadelphia Lippincott Williams & Wilkins; 2005. Shoulder injuries; p. 1033.
-
- Simon R.R.S.S., Koenigsknecht S.J. McGraw-Hill; New York: 2006. Emergency Orthopedics: The Extremities.
-
- Simonet W.T., Melton L.J., Cofield R.H., Ilstrup D.M. Incidence of anterior shoulder dislocation in Olmsted County, Minnesota. Clin Orthop Relat Res. 1984;1984(186):186–191. - PubMed
-
- Sineff S.S.R.E. Shoulder joint dislocation reduction. In: Reichman E.F.S.R., editor. Emergency Medicine Procedures. McGraw-Hill; New-York: 2004. p. 593.
-
- Zacchilli M. a, Owens BD. Epidemiology of shoulder dislocations presenting to emergency departments in the United States. J Bone Jt Surg Am. 2010;92(3):542–549. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
