

Treatment Burden of Medicare Beneficiaries With Stage I Non-Small-Cell Lung Cancer
- PMID: 27997301
- PMCID: PMC5659117
- DOI: 10.1200/JOP.2016.014100
Treatment Burden of Medicare Beneficiaries With Stage I Non-Small-Cell Lung Cancer
Erratum in
-
Errata.J Oncol Pract. 2017 Nov;13(11):776. doi: 10.1200/JOP.2017.028316. J Oncol Pract. 2017. PMID: 29125927 Free PMC article. No abstract available.
Abstract
Purpose: To quantify the burden and complexity associated with treatment of Medicare beneficiaries with stage I non-small-cell lung cancer (NSCLC).
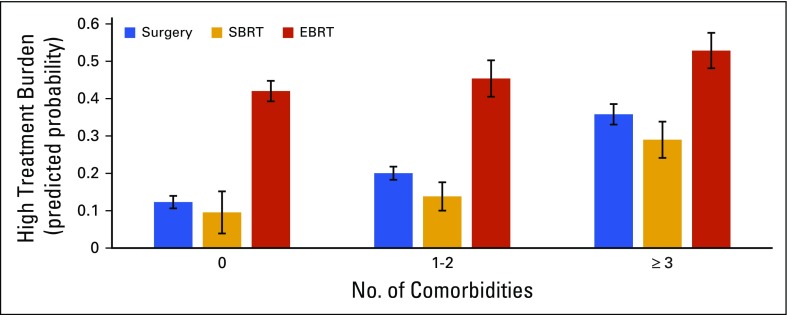
Methods: Using the SEER-Medicare database, we conducted a retrospective cohort study of Medicare beneficiaries who were diagnosed with stage I NSCLC from 2007 to 2011 and who were treated with surgery, stereotactic body radiation therapy, or external beam radiation therapy. Main outcome measures were the number of days a patient was in contact with the health care system (encounter days), the number of physicians involved in a patient's care, and the number of medications prescribed. Logistic regression modeled the association between patient characteristics, treatment type, and high treatment burden (defined as ≥ 66 encounter days).
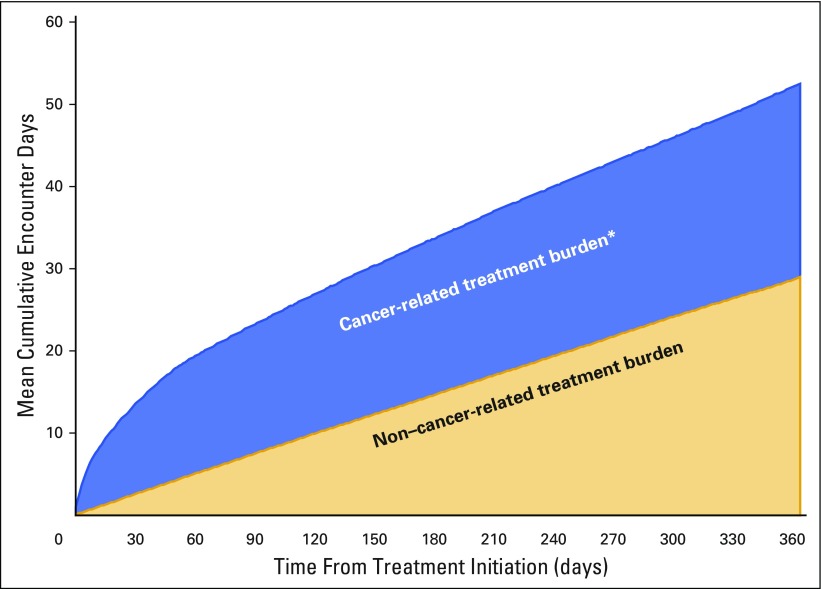
Results: On average, 7,955 patients spent 1 in 3 days interacting with the health care system during the initial 60 days of treatment. Patients experienced a median of 44 encounter days with high variability (interquartile range [IQR], 29 to 66) in the 12 months after treatment initiation. The median number of physicians involved was 20 (IQR, 14 to 28), and the median number of medications prescribed was 12 (IQR, 8 to 17). Patients who were treated with surgery had high treatment burden (predicted probability, 21.6%; 95% CI, 20.2 to 23.1) compared with patients who were treated with stereotactic body radiation therapy (predicted probability, 16.1%; 95% CI, 12.9 to 19.3), whereas patients who were treated with external beam radiation therapy had the highest burden (predicted probability, 46.8%; 95% CI, 43.3 to 50.2).
Conclusion: The treatment burden imposed on patients with early-stage NSCLC was substantial in terms of the number of encounters, physicians involved, and medications prescribed. Because treatment burden varied markedly across patients and treatment types, future work should identify opportunities to understand and ameliorate this burden.
Figures
Comment in
-
Curing Early-Stage Lung Cancer: Is There an Easy Way Out?J Oncol Pract. 2017 Feb;13(2):63-65. doi: 10.1200/JOP.2016.018309. Epub 2016 Dec 20. J Oncol Pract. 2017. PMID: 27997303 No abstract available.
References
-
- Henry DH, Viswanathan HN, Elkin EP, et al. Symptoms and treatment burden associated with cancer treatment: Results from a cross-sectional national survey in the U.S. Support Care Cancer. 2008;16:791–801. - PubMed
-
- May C, Montori VM, Mair FS. We need minimally disruptive medicine. BMJ. 2009;339:b2803. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
