

Exploring the Relationship Between Patient Age and Cancer-Specific Survival in Papillary Thyroid Cancer: Rethinking Current Staging Systems
- PMID: 27998233
- PMCID: PMC6366247
- DOI: 10.1200/JCO.2016.68.9372
Exploring the Relationship Between Patient Age and Cancer-Specific Survival in Papillary Thyroid Cancer: Rethinking Current Staging Systems
Abstract
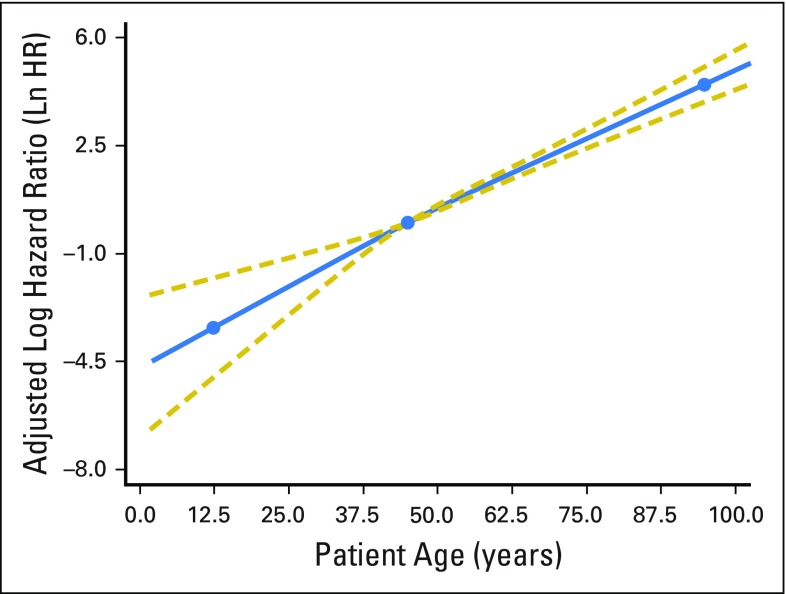
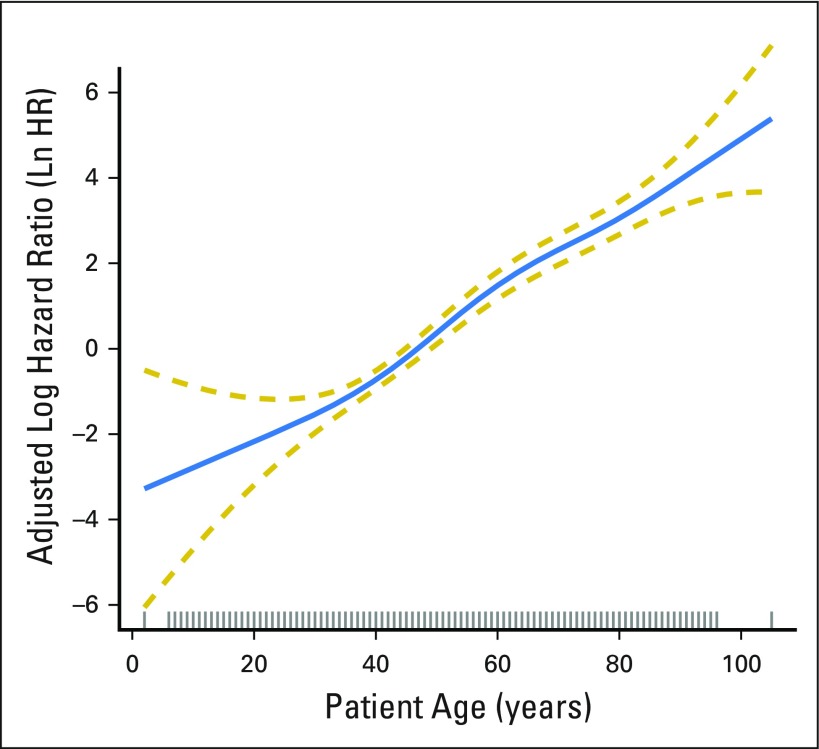
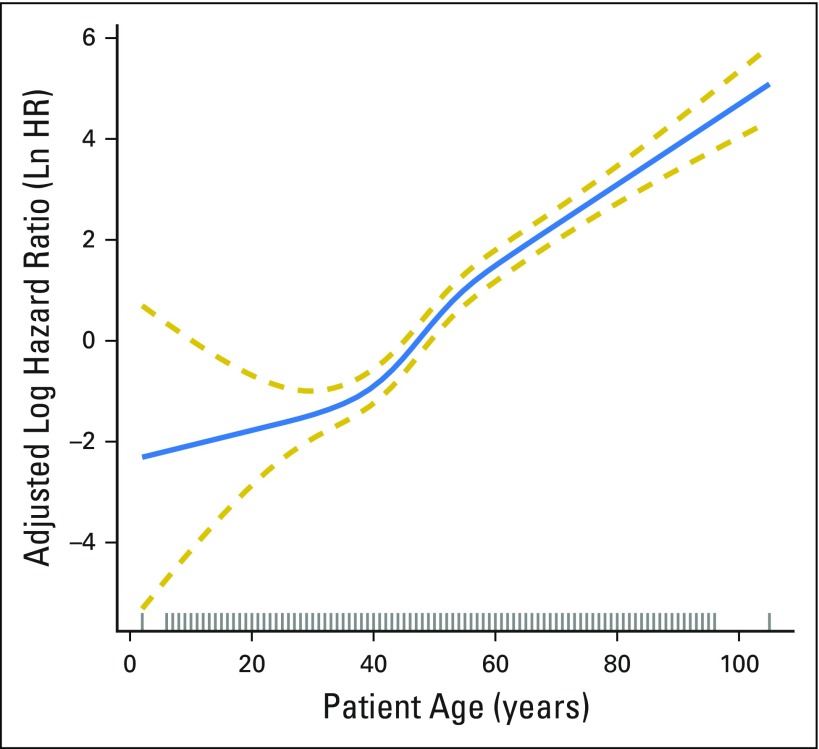
Purpose Patient age is considered to play a unique prognostic role in papillary thyroid cancer (PTC), with a distinct staging dichotomization at 45 years of age. This is based on older, limited data demonstrating a marked rise in mortality around the ages of 40 to 50 years. We hypothesized that age is associated with compromised survival from cancer, with no cutoff denoting survival difference. Patients and Methods Patients with PTC who had surgery were identified from the SEER database (1998 to 2012). Multivariable proportional hazards modeling utilizing several flexible smoothing approaches were used to examine the association between age and cancer-specific survival (CSS) and to determine whether there is an age cut point that is associated with CSS decrement. Results A total of 31,802 patients with PTC were included. Median age was 45 years (range, 2 to 105 years). Ten-year CSS according to age was as follows: 2 to 19 years, 99.8%; 20 to 29 years, 99.9%; 30 to 39 years, 99.8%; 40 to 49 years, 99.5%; 50 to 59 years, 98.1%; 60 to 69 years, 94.8%; 70 to 79 years, 91.5%; 80 to 89 years, 79.2%; and ≥ 90 years, 73.9%. After adjustment for patient demographic and clinicopathologic characteristics, increasing age was associated with increasing mortality from the disease in a dose-dependent fashion, without an apparent cut point. Each of the smoothing approaches demonstrated a similar linearity of risk over all ages and provided close measures of goodness of fit to the data. Conclusion Patient age is significantly associated with death from PTC in a linear fashion, without an apparent age cut point demarcating survival difference. These results challenge the appropriateness of a patient age cut point in current staging systems for PTC and argue for considering a revision in how we anticipate prognosis for patients with PTC.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at
Figures
References
-
- American Cancer Society: Cancer facts & figures 2015. Atlanta: American Cancer Society, 2015. http://www.cancer.org/acs/groups/content/@research/documents/document/ac....
-
- Desquilbet L, Mariotti F. Dose-response analyses using restricted cubic spline functions in public health research. Stat Med. 2010;29:1037–1057. - PubMed
-
- Aschebrook-Kilfoy B, Kaplan EL, Chiu BC, et al. The acceleration in papillary thyroid cancer incidence rates is similar among racial and ethnic groups in the United States. Ann Surg Oncol. 2013;20:2746–2753. - PubMed
-
- Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA. 2006;295:2164–2167. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
