

Review of the Diagnostic Evaluation of Renal Tubular Acidosis
- PMID: 27999512
- PMCID: PMC5158160
Review of the Diagnostic Evaluation of Renal Tubular Acidosis
Abstract
Background: The term renal tubular acidosis (RTA) describes a group of uncommon kidney disorders characterized by defective acid-base regulation. Reaching the diagnosis of RTA is complex and often delayed, resulting in suboptimal treatment.
Methods: This article provides an overview of the clinical features of RTA and diagnostic approaches in a format accessible to physicians for everyday use.
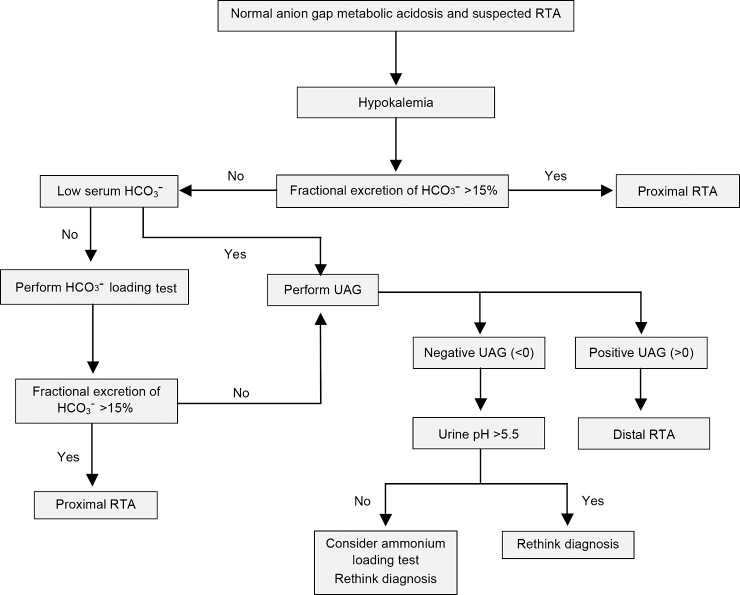
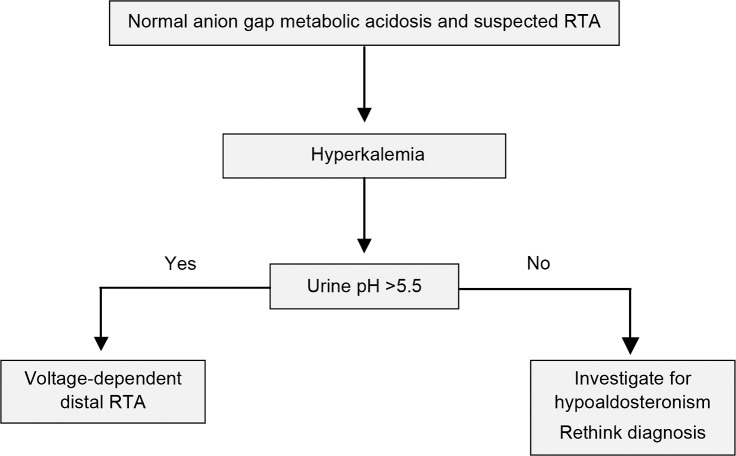
Results: The 3 major forms of disease are classified by their respective tubular transport defects, each of which produces persistent hyperchloremic metabolic acidosis. Distal RTA is characterized by limited urinary acid secretion, proximal RTA by restricted urinary bicarbonate reabsorption, and hyperkalemic RTA by absolute or relative hypoaldosteronism. RTA is often detected incidentally as a biochemical diagnosis in asymptomatic individuals. When present, clinical features may range from mild nonspecific complaints to life-threatening physiologic disturbances.
Conclusion: RTA is a complex condition that requires thoughtful investigation. Physicians should be aware of the presentation of RTA and the investigative options available to confirm the diagnosis.
Keywords: Acid-base equilibrium; acidosis; acidosis–renal tubular.
Figures
References
-
- Rodriguez Soriano J. Renal tubular acidosis: the clinical entity. J Am Soc Nephrol. 2002. August; 13 8: 2160- 2170. - PubMed
-
- Caruana RJ, Buckalew VM., Jr The syndrome of distal (type 1) renal tubular acidosis. Clinical and laboratory findings in 58 cases. Medicine (Baltimore). 1988. March; 67 2: 84- 99. - PubMed
-
- Kurtzman NA. Renal tubular acidosis syndromes. South Med J. 2000. November; 93 11: 1042- 1052. - PubMed
-
- Bökenkamp A, Bökenhauer D, Cheong HI, et al. Dent-2 disease: a mild variant of Lowe syndrome. J Pediatr. 2009. July; 155 1: 94- 99. - PubMed
-
- Rose BD, Post TW. Clinical Physiology of Acid-Base and Electrolyte Disorders. 5th ed. New York, NY: McGraw-Hill; 2001.
Publication types
LinkOut - more resources
Full Text Sources