

Adaptation to microgravity, deconditioning, and countermeasures
- PMID: 28000175
- PMCID: PMC10717636
- DOI: 10.1007/s12576-016-0514-8
Adaptation to microgravity, deconditioning, and countermeasures
Abstract
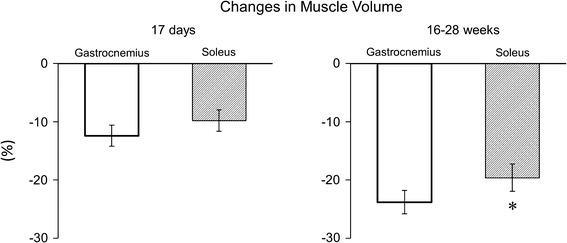
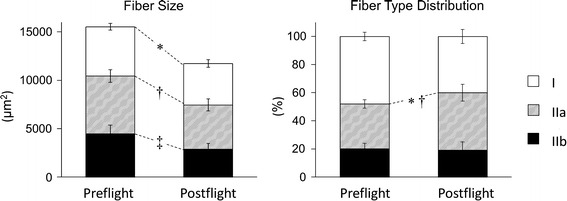
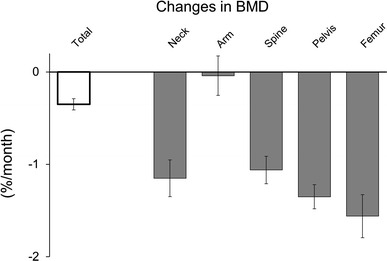
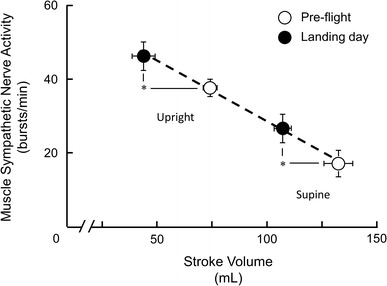
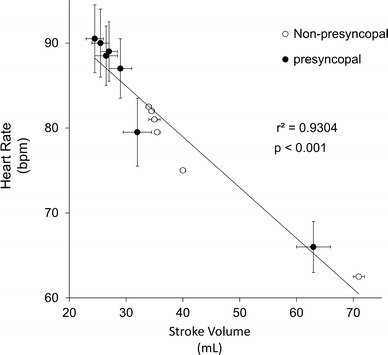
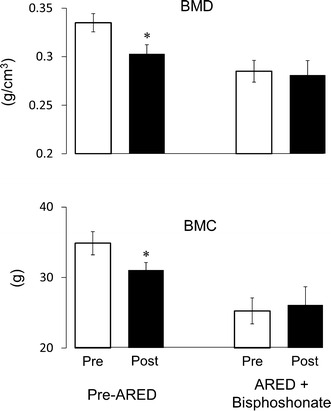
Humans are generally in standing or sitting positions on Earth during the day. The musculoskeletal system supports these positions and also allows motion. Gravity acting in the longitudinal direction of the body generates a hydrostatic pressure difference and induces footward fluid shift. The vestibular system senses the gravity of the body and reflexively controls the organs. During spaceflight or exposure to microgravity, the load on the musculoskeletal system and hydrostatic pressure difference is diminished. Thus, the skeletal muscle, particularly in the lower limbs, is atrophied, and bone minerals are lost via urinary excretion. In addition, the heart is atrophied, and the plasma volume is decreased, which may induce orthostatic intolerance. Vestibular-related control also declines; in particular, the otolith organs are more susceptible to exposure to microgravity than the semicircular canals. Using an advanced resistive exercise device with administration of bisphosphonate is an effective countermeasure against bone deconditioning. However, atrophy of skeletal muscle and the heart has not been completely prevented. Further ingenuity is needed in designing countermeasures for muscular, cardiovascular, and vestibular dysfunctions.
Keywords: Atrophy; Bisphosphonate; Bone mineral density; Gravity; Hydrostatic pressure; Orthostatic intolerance; Spaceflight.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Joseph J. Locomotor system. In: Hamilton WJ, editor. Textbook of human anatomy. London: The macmillan press; 1976.
-
- Kumakura H, Inokuchi S. Lay-out of the human triceps surae muscle: with special concern for the origin of the human bipedal posture. Showa Univ J Med Sci. 1991;3:79–89. doi: 10.15369/sujms1989.3.79. - DOI
-
- Suzuki A, Hayama S. Individual variation in myofiber type composition in the triceps surae and flexor digitorum superficialis. Anthropol Sci. 1994;102(Suppl):127–138. doi: 10.1537/ase.102.Supplement_127. - DOI
-
- Watenpaugh DE, Hargens AR. The cardiovascular system in microgravity. In: Fregly MJ, Blatteis CM, editors. Handbook of physiology, the gravitational environment. Maryland: American Physiological Society; 1996.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
