

Recent technological advances in pediatric brain tumor surgery
- PMID: 28001090
- PMCID: PMC6027926
- DOI: 10.2217/cns-2016-0022
Recent technological advances in pediatric brain tumor surgery
Abstract
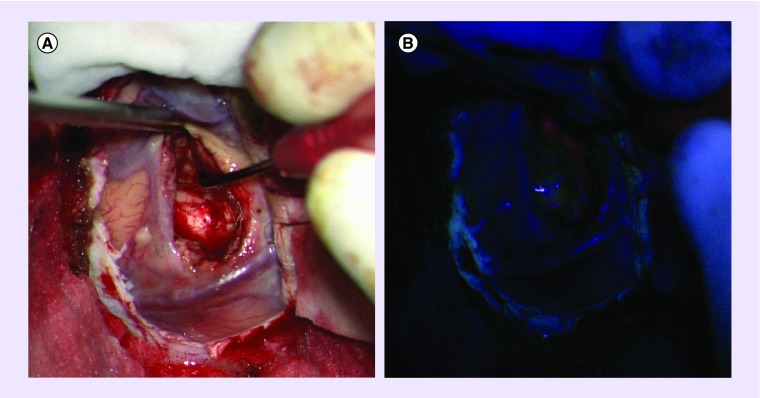
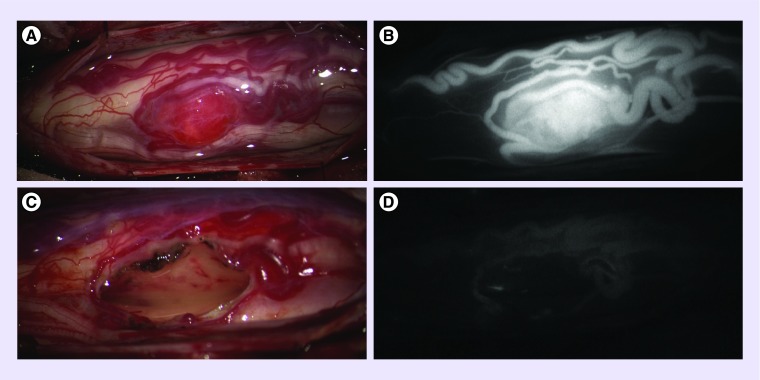
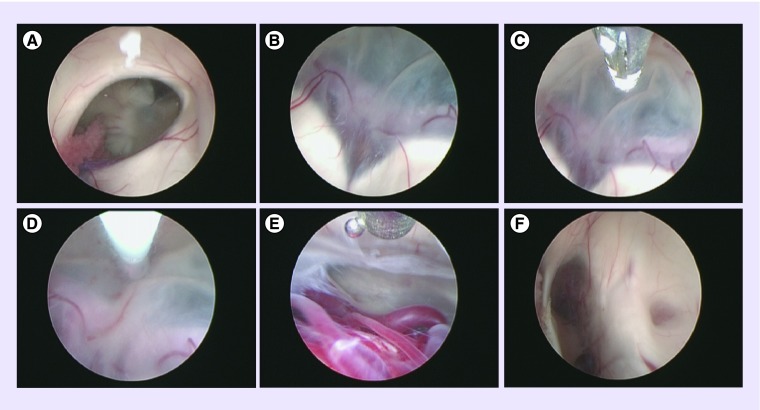
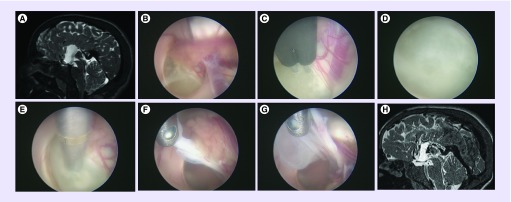
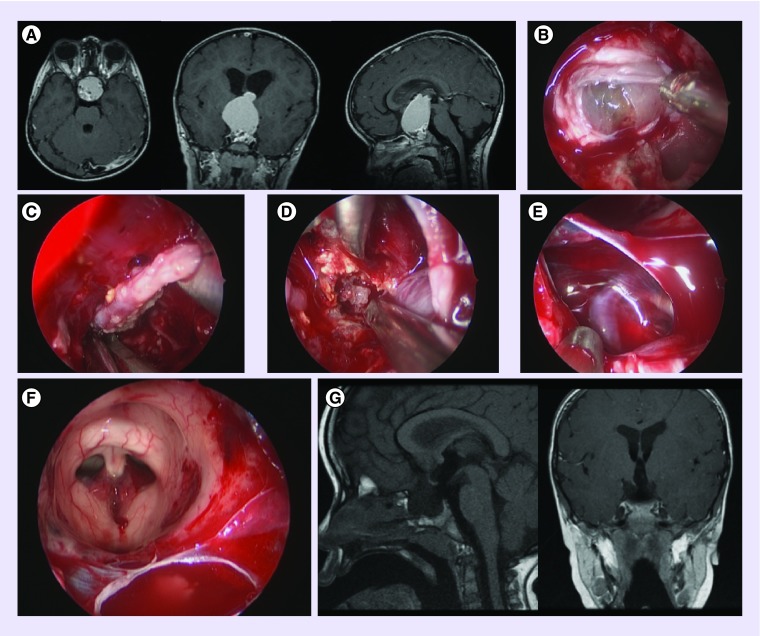
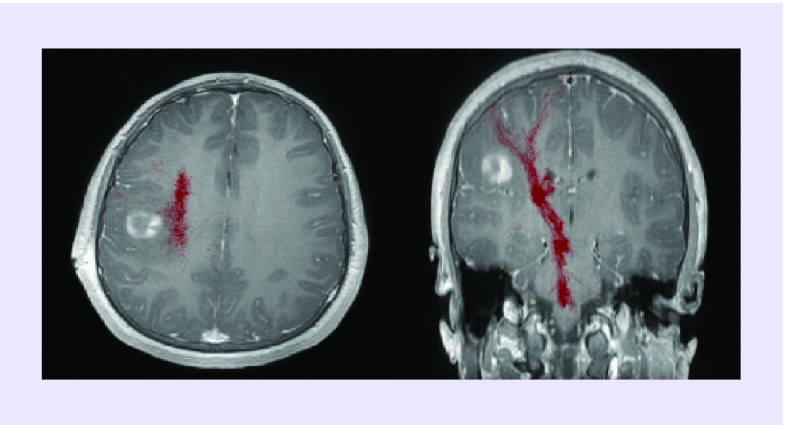
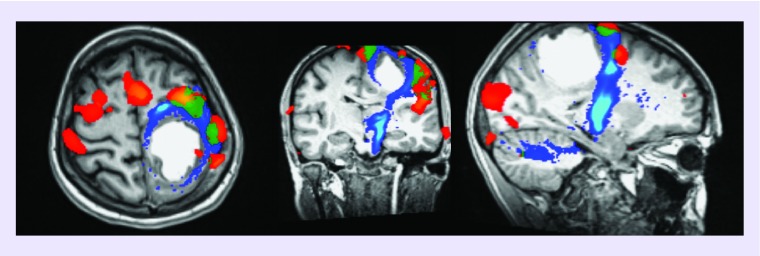
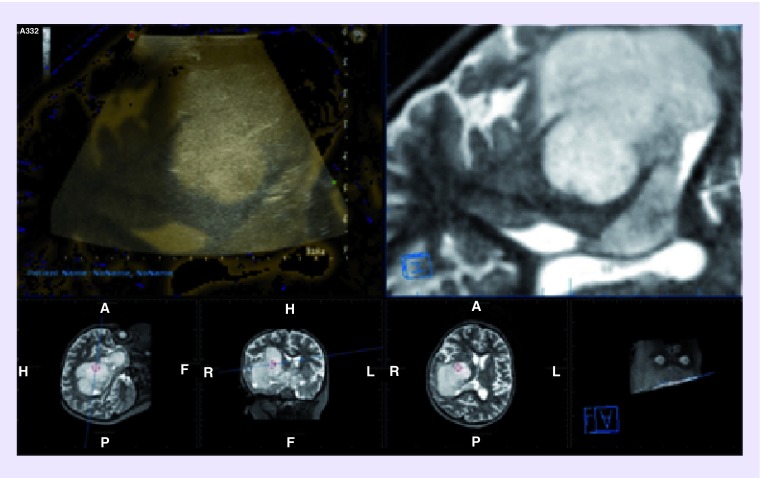
X-rays and ventriculograms were the first imaging modalities used to localize intracranial lesions including brain tumors as far back as the 1880s. Subsequent advances in preoperative radiological localization included computed tomography (CT; 1971) and MRI (1977). Since then, other imaging modalities have been developed for clinical application although none as pivotal as CT and MRI. Intraoperative technological advances include the microscope, which has allowed precise surgery under magnification and improved lighting, and the endoscope, which has improved the treatment of hydrocephalus and allowed biopsy and complete resection of intraventricular, pituitary and pineal region tumors through a minimally invasive approach. Neuronavigation, intraoperative MRI, CT and ultrasound have increased the ability of the neurosurgeon to perform safe and maximal tumor resection. This may be facilitated by the use of fluorescing agents, which help define the tumor margin, and intraoperative neurophysiological monitoring, which helps identify and protect eloquent brain.
Keywords: Brain tumor; endoscope; microscope; paediatric; technological advances.
Conflict of interest statement
Figures
Similar articles
-
Functional Magnetic Resonance Imaging (fMRI), Pre-intraoperative Tractography in Neurosurgery: The Experience of Sant' Andrea Rome University Hospital.Acta Neurochir Suppl. 2017;124:241-250. doi: 10.1007/978-3-319-39546-3_36. Acta Neurochir Suppl. 2017. PMID: 28120080
-
Technical principles in glioma surgery and preoperative considerations.J Neurooncol. 2016 Nov;130(2):243-252. doi: 10.1007/s11060-016-2171-4. Epub 2016 Jun 17. J Neurooncol. 2016. PMID: 27317446 Review.
-
Techniques for Open Surgical Resection of Brain Metastases.Neurosurg Clin N Am. 2020 Oct;31(4):527-536. doi: 10.1016/j.nec.2020.06.003. Epub 2020 Aug 14. Neurosurg Clin N Am. 2020. PMID: 32921349 Review.
-
Intraoperative imaging using a mobile computed tomography scanner.Minim Invasive Neurosurg. 2003 Dec;46(6):317-22. doi: 10.1055/s-2003-812496. Minim Invasive Neurosurg. 2003. PMID: 14968395
-
Impact of Virtual and Augmented Reality Based on Intraoperative Magnetic Resonance Imaging and Functional Neuronavigation in Glioma Surgery Involving Eloquent Areas.World Neurosurg. 2016 Dec;96:375-382. doi: 10.1016/j.wneu.2016.07.107. Epub 2016 Aug 10. World Neurosurg. 2016. PMID: 27521727
Cited by
-
Functional Magnetic Resonance Imaging and Diffusion Tensor Imaging-Tractography in Resective Brain Surgery: Lesion Coverage Strategies and Patient Outcomes.Brain Sci. 2023 Nov 9;13(11):1574. doi: 10.3390/brainsci13111574. Brain Sci. 2023. PMID: 38002534 Free PMC article.
-
Potential biomarkers of childhood brain tumor identified by proteomics of cerebrospinal fluid from extraventricular drainage (EVD).Sci Rep. 2021 Jan 19;11(1):1818. doi: 10.1038/s41598-020-80647-w. Sci Rep. 2021. PMID: 33469081 Free PMC article.
-
Late Effects of Craniospinal Irradiation Using Electron Spinal Fields for Pediatric Patients With Cancer.Int J Radiat Oncol Biol Phys. 2023 Jan 1;115(1):164-173. doi: 10.1016/j.ijrobp.2022.06.055. Epub 2022 Jun 15. Int J Radiat Oncol Biol Phys. 2023. PMID: 35716848 Free PMC article.
-
Intraoperative Neurophysiological Monitoring in Neurosurgery.J Clin Med. 2024 May 17;13(10):2966. doi: 10.3390/jcm13102966. J Clin Med. 2024. PMID: 38792507 Free PMC article. Review.
-
Postoperative Care of Pediatric Brain Tumors: Let's Work Together.Indian J Crit Care Med. 2023 Mar;27(3):161-162. doi: 10.5005/jp-journals-10071-24421. Indian J Crit Care Med. 2023. PMID: 36960116 Free PMC article.
References
-
- Uluç K, Kujoth GC, Başkaya MK. Operating microscopes: past, present, and future. Neurosurg. Focus. 2009;27(3):E4. - PubMed
-
- Stummer W, Pichlmeier U, Meinel T, Wiestler OD, Zanella F, Reulen HJ ALA-Glioma Study Group. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre Phase III trial. Lancet Oncol. 2006;7:392–401. - PubMed
-
- Preuß M, Renner C, Krupp W, et al. The use of 5-aminolevulinic acid fluorescence guidance in resection of pediatric brain tumors. Childs Nerv. Syst. 2013;29:1263–1267. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical