

Differences in Hospital Risk-standardized Mortality Rates for Acute Myocardial Infarction When Assessed Using Transferred and Nontransferred Patients
- PMID: 28002203
- PMCID: PMC5391291
- DOI: 10.1097/MLR.0000000000000691
Differences in Hospital Risk-standardized Mortality Rates for Acute Myocardial Infarction When Assessed Using Transferred and Nontransferred Patients
Abstract
Background: One in 5 patients with acute myocardial infarction (AMI) are transferred between hospitals. However, current hospital performance measures based on AMI mortality exclude these patients from the evaluation of referral hospitals.
Objective: To determine the relationship between risk-standardized mortality for transferred and nontransferred patients at referral hospitals.
Research design: This is a retrospective cohort study.
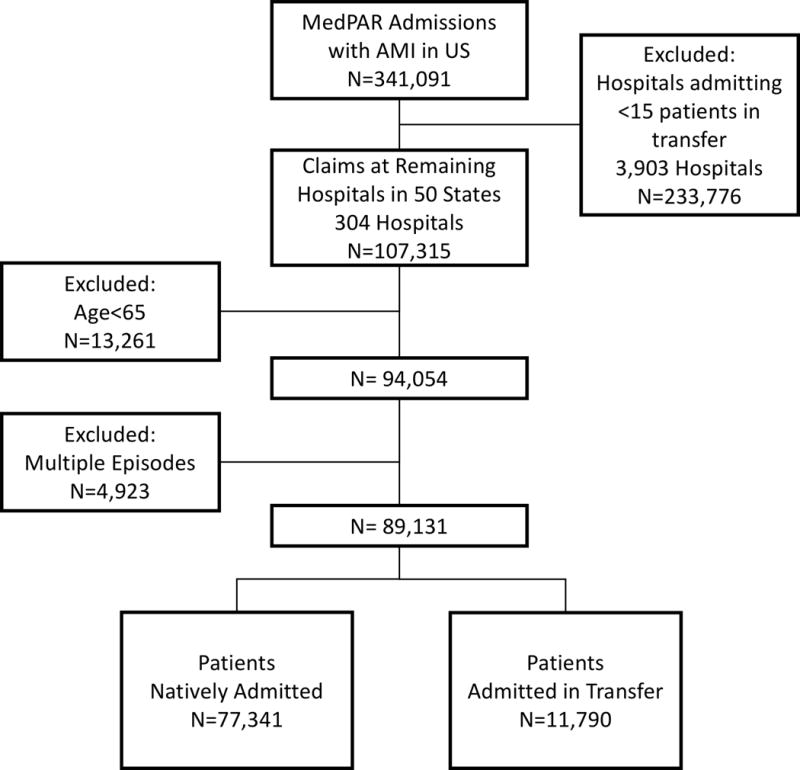
Subjects: Fee-for-service Medicare claims from 2011 for patients hospitalized with a primary diagnosis of AMI, at hospitals admitting at least 15 patients in transfer.
Measures: Hospital-specific risk-standardized 30-day mortality rates (RSMRs) for 2 groups of patients: those admitted through transfer from another hospital, and those natively admitted without a preceding or subsequent interhospital transfer.
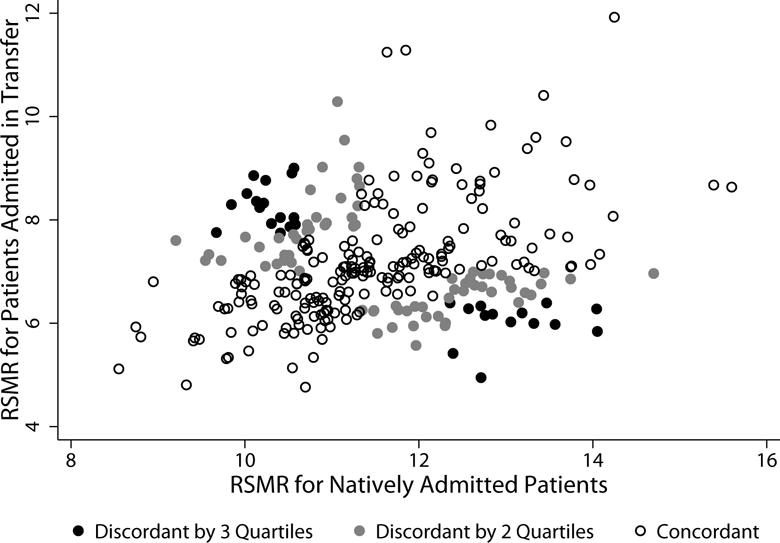
Results: There were 304 hospitals admitting at least 15 patients in transfer. These hospitals cared for 77,711 natively admitted patients (median, 254; interquartile range, 162-321), and 11,829 patients admitted in transfer (median, 26; interquartile range, 19-46). Risk-standardized mortality rates were higher for natively admitted patients than for those admitted in transfer (mean, 11.5%±1.2% vs. 7.2%±1.1%). There was weak correlation between hospital performance as assessed by RSMR for patients natively admitted versus those admitted in transfer (Pearson r=0.24, P<0.001); when performance was arrayed by quartile, 102 hospitals (33.6%) differed at least 2 quartiles of performance across the 2 patient groups.
Conclusions: For Medicare patients with AMI, hospital-specific RSMRs for natively admitted patients are only weakly associated with RSMRs for patients transferred in from another hospital. Current AMI performance metrics may fail to provide guidance about hospital quality for transferred patients.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Krumholz HM, Wang Y, Mattera JA, Wang Y, Han LF, Ingber MJ, et al. An administrative claims model suitable for profiling hospital performance based on 30-day mortality rates among patients with an acute myocardial infarction. Circulation [Internet] 2006;113(13):1683–92. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16549637. - PubMed
-
- Krumholz HM, Wang Y, Mattera JA, Wang Y, Han LF, Ingber MJ, et al. An administrative claims model suitable for profiling hospital performance based on 30-day mortality rates among patients with heart failure. Circulation [Internet] 2006;113(13):1693–701. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16549636. - PubMed
-
- Lindenauer PK, Bernheim SM, Grady JN, Lin Z, Wang Y, Wang Y, et al. The performance of US hospitals as reflected in risk-standardized 30-day mortality and readmission rates for medicare beneficiaries with pneumonia. J Hosp Med. 2010 Aug;5(6):E12–18. - PubMed
-
- Liem AL, van ’t Hof AW, Hoorntje JC, de Boer MJ, Suryapranata H, Zijlstra F. Influence of treatment delay on infarct size and clinical outcome in patients with acute myocardial infarction treated with primary angioplasty. J Am Coll Cardiol [Internet] 1998 Sep;32(3):629–33. [cited 2016 Oct 3] Available from: http://www.ncbi.nlm.nih.gov/pubmed/9741503. - PubMed
-
- Westfall JM, Kiefe CI, Weissman NW, Goudie A, Centor RM, Williams OD, et al. Does interhospital transfer improve outcome of acute myocardial infarction? A propensity score analysis from the Cardiovascular Cooperative Project. BMC Cardiovasc Disord [Internet] 2008;8:22. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18782452. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
