

Reoperation Rates in Ductal Carcinoma In Situ vs Invasive Breast Cancer After Wire-Guided Breast-Conserving Surgery
- PMID: 28002557
- PMCID: PMC5470426
- DOI: 10.1001/jamasurg.2016.4751
Reoperation Rates in Ductal Carcinoma In Situ vs Invasive Breast Cancer After Wire-Guided Breast-Conserving Surgery
Abstract
Importance: New techniques for preoperative localization of nonpalpable breast lesions may decrease the reoperation rate in breast-conserving surgery (BCS) compared with rates after surgery with the standard wire-guided localization. However, a valid reoperation rate for this procedure needs to be established for comparison, as previous studies on this procedure include a variety of malignant and benign breast lesions.
Objectives: To determine the reoperation rate after wire-guided BCS in patients with histologically verified nonpalpable invasive breast cancer (IBC) or ductal carcinoma in situ (DCIS) and to examine whether the risk of reoperation is associated with DCIS or histologic type of the IBC.
Design, setting, and participants: This nationwide study including women with histologically verified IBC or DCIS having wire-guided BCS performed between January 1, 2010, and December 31, 2013, used data from the Danish National Patient Registry that were cross-checked with the Danish Breast Cancer Group database and the Danish Pathology Register.
Main outcomes and measures: Reoperation rate after wire-guided BCS in patients with IBC or DCIS.
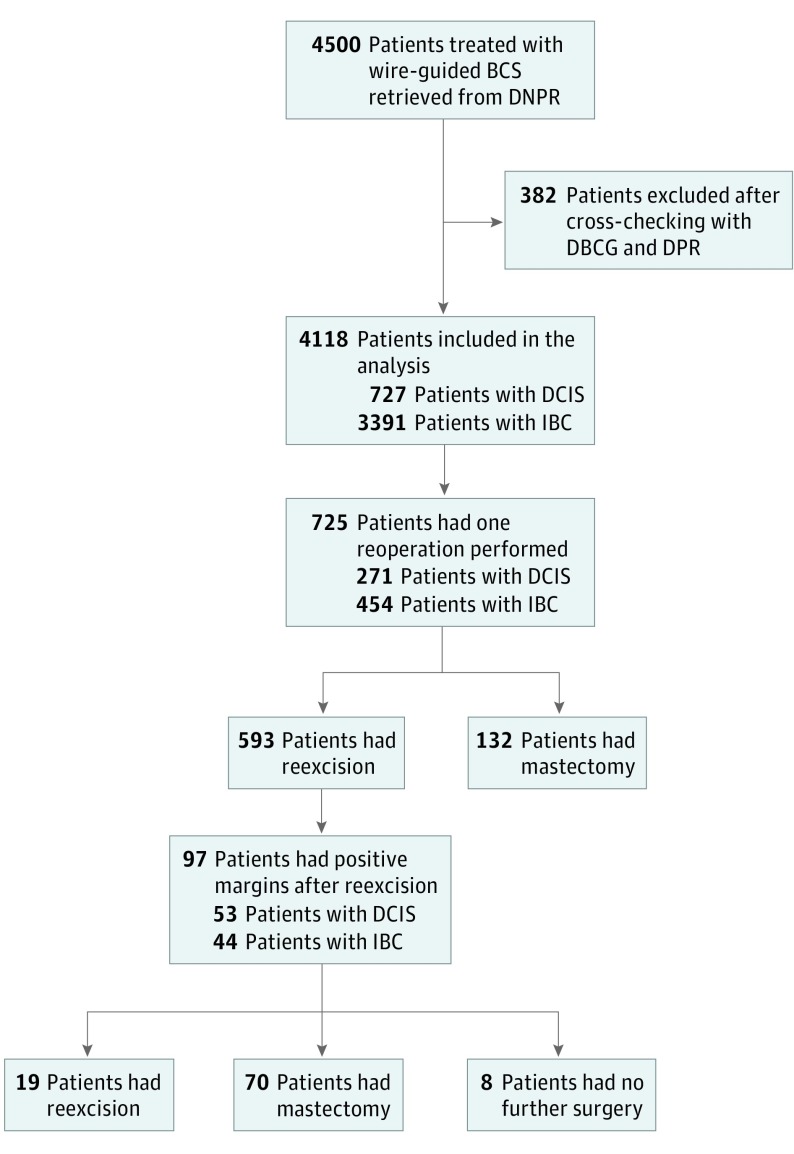
Results: Wire-guided BCS was performed in 4118 women (mean [SD] age, 60.9 [8.7] years). A total of 725 patients (17.6%) underwent a reoperation: 593 were reexcisions (14.4%) and 132 were mastectomies (3.2%). Significantly more patients with DCIS (271 of 727 [37.3%]) than with IBC (454 of 3391 [13.4%]) underwent a reoperation (adjusted odds ratio, 3.82; 95% CI, 3.19-4.58; P < .001). After the first reexcision, positive margins were still present in 97 patients (16.4%). The risk of repeated positive margins was significantly higher in patients with DCIS vs those with IBC (unadjusted odds ratio, 2.21; 95% CI, 1.42-3.43; P < .001). The risk of reoperation was significantly increased in patients with lobular carcinoma vs those with ductal carcinoma (adjusted odds ratio, 1.44; 95% CI 1.06-1.95; P = .02). A total of 202 patients (4.9%) had a subsequent completion mastectomy, but no difference was found in the type of reoperation between patients with DCIS and those with IBC.
Conclusions and relevance: A lower reoperation rate after wire-guided BCS was found in this study than those shown in previous studies. However, the risk of reoperation in patients with DCIS was 3 times higher than in those with IBC. The widespread use of mammographic screening will increase the number of patients diagnosed with DCIS, making a precise localization of nonpalpable DCIS lesions even more important.
Conflict of interest statement
Figures
Comment in
-
Difficulty of Achieving Clear Margins in Nonpalpable Ductal Carcinoma of the Breast.JAMA Surg. 2017 Apr 1;152(4):385. doi: 10.1001/jamasurg.2016.4752. JAMA Surg. 2017. PMID: 28002571 No abstract available.
Similar articles
-
Tumor margins that lead to reoperation in breast cancer: A retrospective register study of 4,489 patients.J Surg Oncol. 2022 Mar;125(4):577-588. doi: 10.1002/jso.26749. Epub 2021 Nov 15. J Surg Oncol. 2022. PMID: 34779520 Free PMC article.
-
Predictors of Surgical Margin Following Breast-Conserving Surgery: A Large Population-Based Cohort Study.Ann Surg Oncol. 2016 Dec;23(Suppl 5):627-633. doi: 10.1245/s10434-016-5532-5. Epub 2016 Sep 2. Ann Surg Oncol. 2016. PMID: 27590331 Free PMC article.
-
Surgical outcomes and prognosis of HER2+ invasive breast cancer patients with a DCIS component treated with breast-conserving surgery after neoadjuvant systemic therapy.Eur J Surg Oncol. 2024 Sep;50(9):108465. doi: 10.1016/j.ejso.2024.108465. Epub 2024 Jun 4. Eur J Surg Oncol. 2024. PMID: 38870869
-
Meta-analysis of the effect of preoperative breast MRI on the surgical management of ductal carcinoma in situ.Br J Surg. 2015 Jul;102(8):883-93. doi: 10.1002/bjs.9797. Epub 2015 Apr 28. Br J Surg. 2015. PMID: 25919321 Review.
-
Carcinoma in situ of the female breast. A clinico-pathological, immunohistological, and DNA ploidy study.APMIS Suppl. 2003;(108):1-67. APMIS Suppl. 2003. PMID: 12874968 Review.
Cited by
-
Predictors of Reexcision following Breast-Conserving Surgery for Ductal Carcinoma In Situ.Ann Surg Oncol. 2021 Mar;28(3):1390-1397. doi: 10.1245/s10434-020-09101-5. Epub 2020 Sep 10. Ann Surg Oncol. 2021. PMID: 32914389
-
Development of intraoperative assessment of margins in breast conserving surgery: a narrative review.Gland Surg. 2022 Jan;11(1):258-269. doi: 10.21037/gs-21-652. Gland Surg. 2022. PMID: 35242687 Free PMC article. Review.
-
Association Between Surgery Preference and Receipt in Ductal Carcinoma In Situ After Breast Magnetic Resonance Imaging: An Ancillary Study of the ECOG-ACRIN Cancer Research Group (E4112).JAMA Netw Open. 2022 May 2;5(5):e2210331. doi: 10.1001/jamanetworkopen.2022.10331. JAMA Netw Open. 2022. PMID: 35536580 Free PMC article.
-
Intraoperative fluorescence imaging with aminolevulinic acid detects grossly occult breast cancer: a phase II randomized controlled trial.Breast Cancer Res. 2021 Jul 12;23(1):72. doi: 10.1186/s13058-021-01442-7. Breast Cancer Res. 2021. PMID: 34253233 Free PMC article. Clinical Trial.
-
Preoperative non-palpable breast lesion localization, innovative techniques and clinical outcomes in surgical practice: A systematic review and meta-analysis.Breast. 2021 Aug;58:93-105. doi: 10.1016/j.breast.2021.04.007. Epub 2021 Apr 22. Breast. 2021. PMID: 33991806 Free PMC article.
References
-
- Vejborg I, Mikkelsen E, Garne JP, et al. . Mammography screening in Denmark. Dan Med Bull. 2011;58(6):C4287. - PubMed
-
- Bleyer A, Welch HG. Effect of three decades of screening mammography on breast-cancer incidence. N Engl J Med. 2012;367(21):1998-2005. - PubMed
-
- Cheung S, Booth ME, Kearins O, Dodwell D. Risk of subsequent invasive breast cancer after a diagnosis of ductal carcinoma in situ (DCIS). Breast. 2014;23(6):807-811. - PubMed
-
- Dansk Kvalitetsdatabase for Mammografiscreening Arsrapport 2014: Tredje nationale screeningsrunde. https://www.sundhed.dk/content/cms/78/4678_dkms-rapport-version-4_final_.... Accessed January 11, 2016.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
