

Outcomes from massive paracetamol overdose: a retrospective observational study
- PMID: 28002875
- PMCID: PMC5427245
- DOI: 10.1111/bcp.13214
Outcomes from massive paracetamol overdose: a retrospective observational study
Abstract
Linked article: This article is commented on by Bateman DN and Dear JW. Should we treat very large paracetamol overdose differently? Br J Clin Pharmacol 2017; 83: 1163-5. https://doi.org/10.1111/bcp.13279 AIMS: Treatment of paracetamol (acetaminophen) overdose with acetylcysteine is standardized, with dose determined only by patient weight. The validity of this approach for massive overdoses has been questioned. We systematically compared outcomes in massive and non-massive overdoses, to guide whether alternative treatment strategies should be considered, and whether the ratio between measured timed paracetamol concentrations (APAPpl ) and treatment nomogram thresholds at those time points (APAPt ) provides a useful assessment tool.
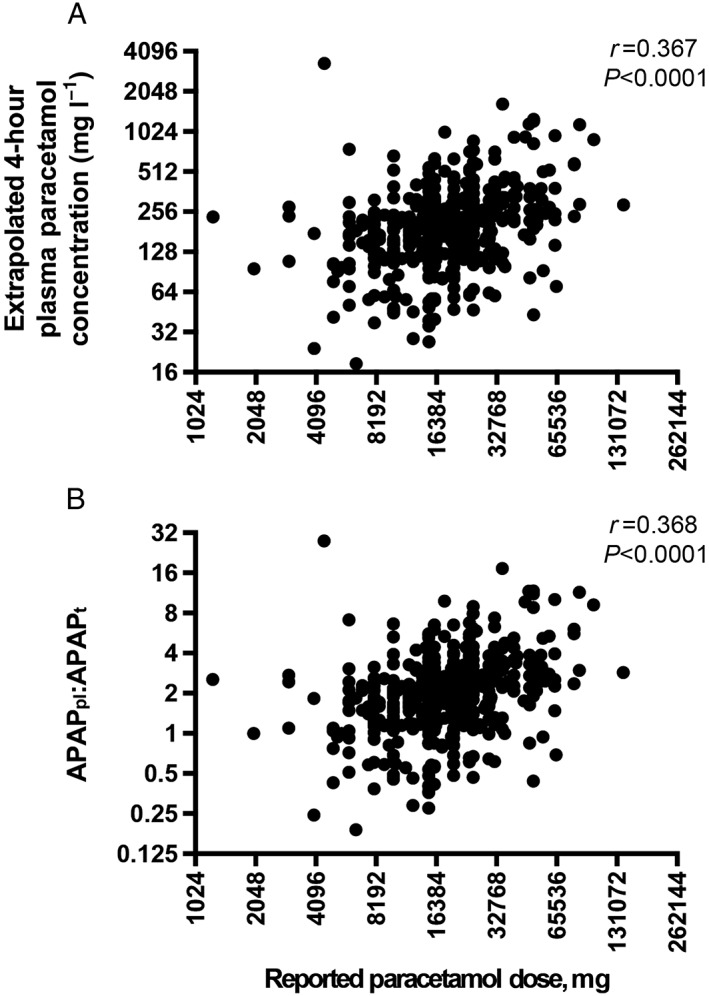
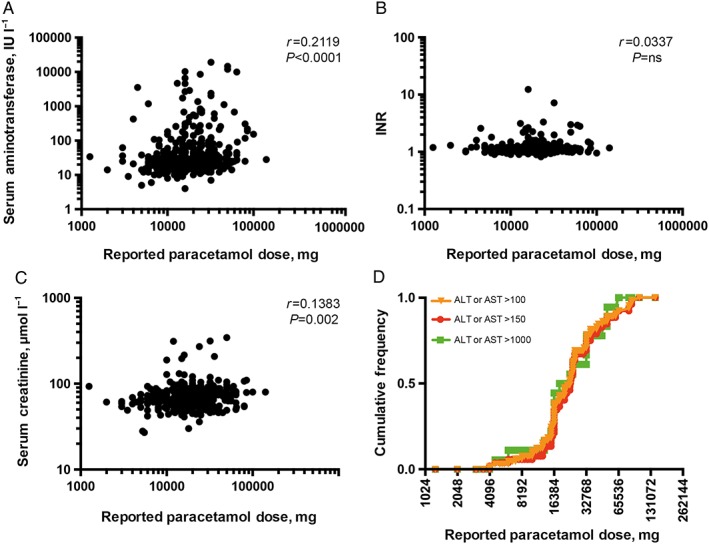
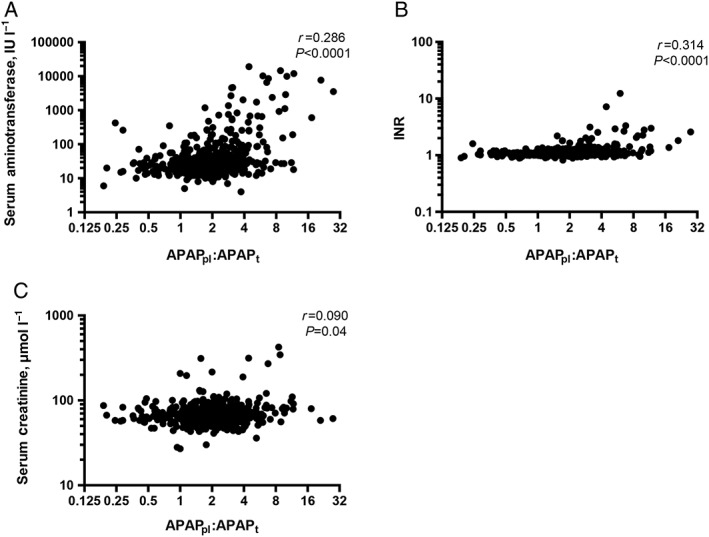
Methods: This is a retrospective observational study of all patients (n = 545) between 2005 and 2013 admitted to a tertiary care toxicology service with acute non-staggered paracetamol overdose. Massive overdoses were defined as extrapolated 4-h plasma paracetamol concentrations >250 mg l-1 , or reported ingestions ≥30 g. Outcomes (liver injury, coagulopathy and kidney injury) were assessed in relation to reported dose and APAPpl :APAPt ratio (based on a treatment line through 100 mg l-1 at 4 h), and time to acetylcysteine.
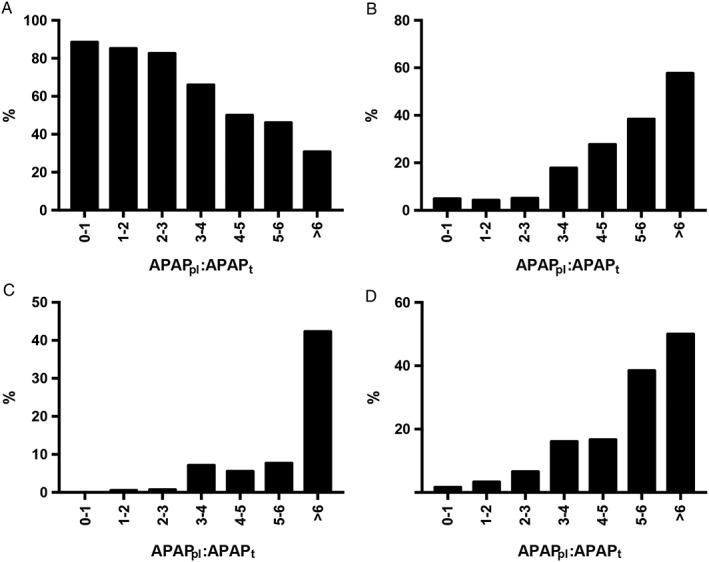
Results: Ingestions of ≥30 g paracetamol correlated with higher peak serum aminotransferase (r = 0.212, P < 0.0001) and creatinine (r = 0.138, P = 0.002) concentrations. Acute liver injury, hepatotoxicity and coagulopathy were more frequent with APAPpl :APAPt ≥ 3 with odds ratios (OR) and 95% confidence intervals (CI) of 9.19 (5.04-16.68), 35.95 (8.80-158.1) and 8.34 (4.43-15.84), respectively (P < 0.0001). Heightened risk persisted in patients receiving acetylcysteine within 8 h of overdose.
Conclusion: Patients presenting following massive paracetamol overdose are at higher risk of organ injury, even when acetylcysteine is administered early. Enhanced therapeutic strategies should be considered in those who have an APAPpl :APAPt ≥ 3. Novel biomarkers of incipient liver injury and abbreviated acetylcysteine regimens require validation in this patient cohort.
Keywords: acetylcysteine; coagulopathy; hepatotoxicity; overdose; paracetamol.
© 2016 The British Pharmacological Society.
Figures
Comment in
-
Should we treat very large paracetamol overdose differently?Br J Clin Pharmacol. 2017 Jun;83(6):1163-1165. doi: 10.1111/bcp.13279. Epub 2017 Apr 5. Br J Clin Pharmacol. 2017. PMID: 28252212 Free PMC article. No abstract available.
References
-
- Larson AM, Polson J, Fontana RJ, Davern TJ, Lalani E, Hynan LS, et al. Acetaminophen‐induced acute liver failure: results of a United States multicenter, prospective study. Hepatology 2005; 42: 1364–1372. - PubMed
-
- Lancaster EM, Hiatt JR, Zarrinpar A. Acetaminophen hepatotoxicity: an updated review. Arch Toxicol 2015; 89: 193–199. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
