

Prescription of renin-angiotensin system blockers and risk of acute kidney injury: a population-based cohort study
- PMID: 28003286
- PMCID: PMC5223684
- DOI: 10.1136/bmjopen-2016-012690
Prescription of renin-angiotensin system blockers and risk of acute kidney injury: a population-based cohort study
Abstract
Objective: To investigate whether there is an association between use of ACE inhibitors (ACEI) and angiotensin receptor blockers (ARB) and risk of acute kidney injury (AKI).
Study design: We conducted a new-user cohort study of the rate of AKI among users of common antihypertensives.
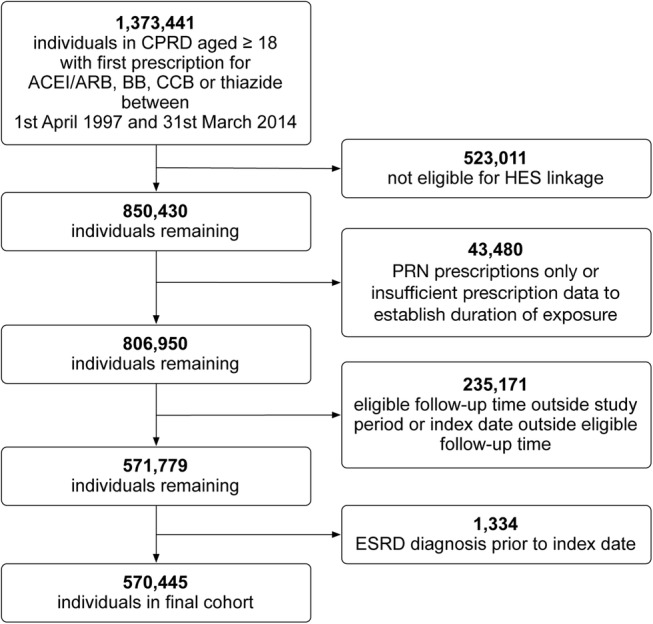
Setting: UK primary care practices contributing to the Clinical Practice Research Datalink (CPRD) eligible for linkage to hospital records data from the Hospital Episode Statistics (HES) database between April 1997 and March 2014.
Participants: New users of antihypertensives: ACEI/ARB, β-blockers, calcium channel blockers and thiazide diuretics.
Outcomes: The outcome was first episode of AKI. We estimated incidence rate ratio (RR) for AKI during time exposed to ACEI/ARB compared to time unexposed, adjusting for age, sex, comorbidities, use of other antihypertensive drugs and calendar period using Poisson regression. Covariates were time updated.
Results: Among 570 445 participants, 303 761 were prescribed ACEI/ARB with a mean follow-up of 4.1 years. The adjusted RR of AKI during time exposed to ACEI/ARB compared to time unexposed was 1.12 (95% CI 1.07 to 1.17). This relative risk varied depending on absolute risk of AKI, with lower or no increased relative risk from the drugs among those at greatest absolute risk. For example, among people with stage 4 chronic kidney disease (who had 6.69 (95% CI 5.57 to 8.03) times higher rate of AKI compared to those without chronic kidney disease), the adjusted RR of AKI during time exposed to ACEI/ARB compared to time unexposed was 0.66 (95% CI 0.44 to 0.97) in contrast to 1.17 (95% CI 1.09 to 1.25) among people without chronic kidney disease.
Conclusions: Treatment with ACEI/ARB is associated with only a small increase in AKI risk while individual patient characteristics are much more strongly associated with the rate of AKI. The degree of increased risk varies between patient groups.
Keywords: acute kidney injury; angiotensin receptor antagonists; angiotensin-converting enzyme inhibitors; cohort study; renin-angiotensin system.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures

References
-
- Think Kidneys. Acute kidney injury: the NHS campaign to improve the care of people at risk of, or with, acute kidney injury, 2016. https://www.thinkkidneys.nhs.uk/aki/ (accessed Jan 2016).
-
- Schoolwerth AC, Sica DA, Ballermann BJ et al. Renal considerations in angiotensin converting enzyme inhibitor therapy: a statement for healthcare professionals from the Council on the Kidney in Cardiovascular Disease and the Council for High Blood Pressure Research of the American Heart Association. Circulation 2001;104:1985–91. 10.1161/hc4101.096153 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous