

Current Status and Future Prospects for Esophageal Cancer Treatment
- PMID: 28003586
- PMCID: PMC5347481
- DOI: 10.5761/atcs.ra.16-00162
Current Status and Future Prospects for Esophageal Cancer Treatment
Abstract
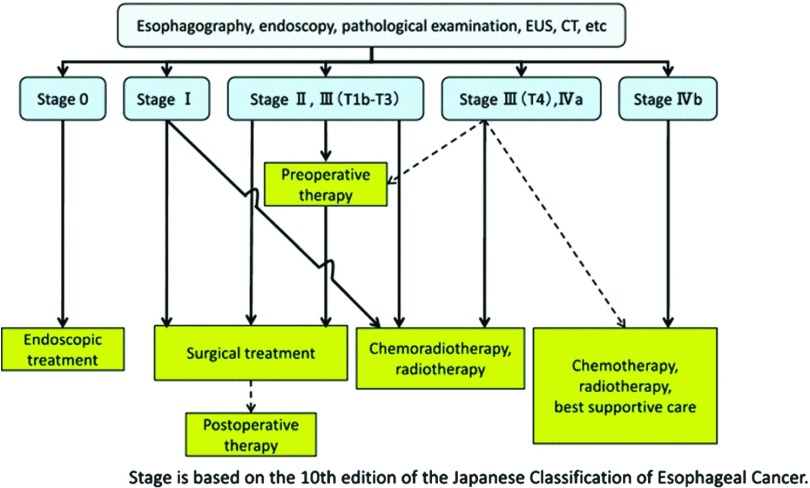
The local control effect of esophagectomy with three-field lymph node dissection (3FLD) is reaching its limit pending technical advancement. Minimally invasive esophagectomy (MIE) by thoracotomy is slowly gaining acceptance due to advantages in short-term outcomes. Although the evidence is slowly increasing, MIE is still controversial. Also, the results of treatment by surgery alone are limiting, and multimodality therapy, which includes surgical and non-surgical treatment options including chemotherapy, radiotherapy, and endoscopic treatment, has become the mainstream therapy. Esophagectomy after neoadjuvant chemotherapy (NAC) is the standard treatment for clinical stages II/III (except for T4) esophageal cancer, whereas chemoradiotherapy (CRT) is regarded as the standard treatment for patients who wish to preserve their esophagus, those who refuse surgery, and those with inoperable disease. CRT is also usually selected for clinical stage IV esophageal cancer. On the other hand, with the spread of CRT, salvage esophagectomy has traditionally been recognized as a feasible option; however, many clinicians oppose the use of surgery due to the associated unfavorable morbidity and mortality profile. In the future, the improvement of each treatment result and the establishment of individual strategies are important although esophageal cancer has many treatment options.
Figures
References
-
- Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin 2011; 61: 69-90. - PubMed
-
- Sato Y, Motoyama S, Takano H, et al. Esophageal Cancer Patients Have a High Incidence of Severe Periodontitis and Preoperative Dental Care Reduces the Likelihood of Severe Pneumonia after Esophagectomy. Dig Surg 2016; 33: 495-502. - PubMed
-
- Ando N, Kato H, Igaki H, et al. A randomized trial comparing postoperative adjuvant chemotherapy with cisplatin and 5-fluorouracil versus preoperative chemotherapy for localized advanced squamous cell carcinoma of the thoracic esophagus (JCOG9907). Ann Surg Oncol 2012; 19: 68-74. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials