

A patient-preference cohort study of office versus inpatient uterine polyp treatment for abnormal uterine bleeding
- PMID: 28003798
- PMCID: PMC5133274
- DOI: 10.1007/s10397-016-0946-4
A patient-preference cohort study of office versus inpatient uterine polyp treatment for abnormal uterine bleeding
Abstract
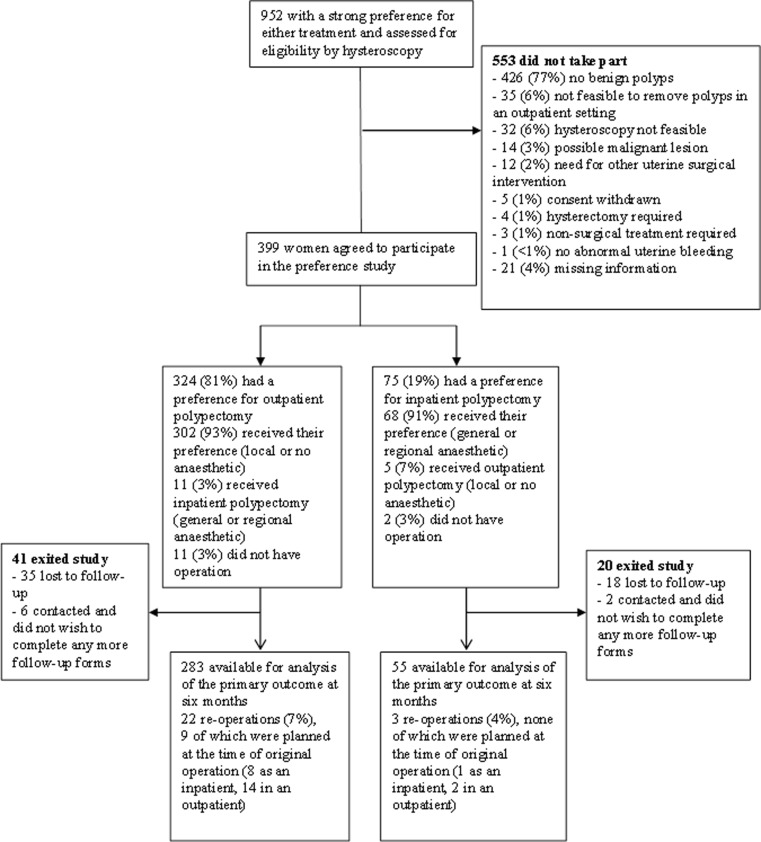
Uterine polyps can cause abnormal bleeding in women. Conventional practise is to remove them under general anaesthesia but advances in technology have made it possible to perform polypectomy in the office setting. We conducted a patient-preference study to explore women's preferences for treatment setting and to evaluate the effectiveness and treatment experience of women undergoing uterine polypectomy. Three hundred ninety-nine women with abnormal uterine bleeding who were found to have uterine polyps at diagnostic hysteroscopy were recruited. Office polypectomies were performed in office hysteroscopy clinics, and inpatient procedures were undertaken in operating theatres. Three hundred twenty-four of 399 (81 %) expressed a preference for office treatment. There was no difference found between office treatment and inpatient treatment in terms of alleviating abnormal uterine bleeding as assessed by patients and in improving disease-specific quality of life. Acceptability was lower and patient pain scores were significantly higher in the office group. When offered a choice of treatment setting for uterine polypectomy, patients have a preference for office over inpatient treatment. Ambulatory gynaecology services should be available within healthcare systems to meet patient demand.
Keywords: Abnormal uterine bleeding; Ambulatory gynaecology; Office polypectomy; Patient preference; Uterine polyp.
Conflict of interest statement
All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf. Prof Clark reports separate research grants from Hologic (formerly Cytyc) and Smith & Nephew to conduct clinical trials in ambulatory care; and honoraria for training and lecturing and travel expenses from the following instrument manufacturers who produce health technologies that can be used in ambulatory care; Ethicon Women’s Health; Hologic; Smith & Nephew; Conceptus; Bayer. Dr. Smith reports a grant from Smith & Nephew, during the conduct of the study, for a trial comparing techniques for office polypectomy. All other authors report no conflicts of interest. Consent All persons gave their informed consent prior to their inclusion in the study. Funding The study sponsors were the University of Birmingham and Birmingham Women’s NHS Foundation Trust, and the study was funded by the National Institute of Health Research (NIHR) Health Technology Assessment Programme (06/404/84). The views and opinions expressed in this article are those of the authors and do not necessarily reflect those of the NIHR Health Technology Assessment Programme, the NIHR, the National Health Service or the English Department of Health. Role of the funding source Neither the funder nor sponsor had any role in study design, data collection, interpretation or analysis or in writing the report for publication. The authors had full access to all the data from the study. The authors vouch for the accuracy and completeness of the data and analyses. Data The corresponding author affirms that the manuscript is an honest, accurate and transparent account of the study being reported that no important aspects of the study have been omitted and that any discrepancies from the study as planned (and, if relevant, registered) have been explained. The full dataset is available from the corresponding author. Consent was not obtained but the presented data are anonymised and risk of identification is low. Ethical approval Ethical approval was obtained from the South West Research Ethics Committee on 15th February 2008. Reference number: 08/H0206/6.
Figures
References
-
- Bradlow J, Coulter A, Brooks P. Patterns of referral. Oxford: Oxford Health Services Research Unit; 1992.
-
- Clevenger-Hoeft M, Syrop CH, Stovall DW, Van Voorhis BJ. Sonohysterography in premenopausal women with and without abnormal bleeding. Obstet Gynecol. 1999;94(4):516–520. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources