

Retention of laparoscopic psychomotor skills after a structured training program depends on the quality of the training and on the complexity of the task
- PMID: 28003800
- PMCID: PMC5133276
- DOI: 10.1007/s10397-016-0962-4
Retention of laparoscopic psychomotor skills after a structured training program depends on the quality of the training and on the complexity of the task
Abstract
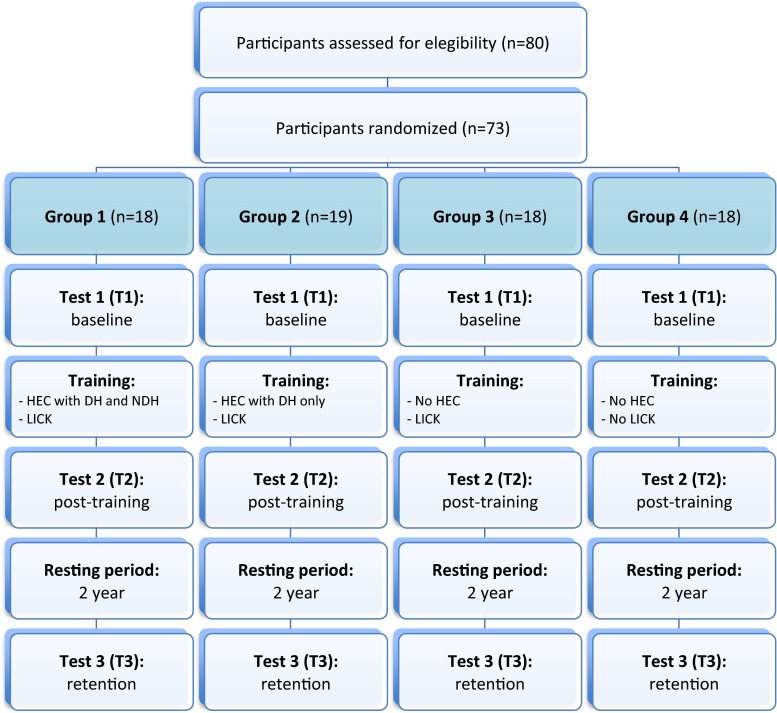
This follow-up RCT was conducted to evaluate laparoscopic psychomotor skills retention after finishing a structured training program. In a first study, 80 gynecologists were randomly allocated to four groups to follow different training programs for hand-eye coordination (task 1) with the dominant hand (task 1-a) and the non-dominant hand (task 1-b) and laparoscopic intra-corporeal knot tying (task 2) in the Laparoscopic Skills Testing and Training (LASTT) model. First, baseline skills were tested (T1). Then, participants trained task 1 (G1: 1-a and 1-b, G2: 1-a only, G3 and G4: none) and then task 2 (all groups but G4). After training all groups were tested again to evaluate skills acquisition (T2). For this study, 2 years after a resting period, 73 participants were recruited and tested again to evaluate skills retention (T3). All groups had comparable skills at T1 for all tasks. At T2, G1, G2, and G3 improved their skills, but the level of improvement was different (G1 = G2 > G3 > G4 for task 1; G1 = G2 = G3 > G4 for task 2). At T3, all groups retained their task 1 skills at the same level than at T2. For task 2, however, a skill decay was already noticed for G2 and G3, being G1 the only group that retained their skills at the post-training level. Training improves laparoscopic skills, which can be retained over time depending on the comprehensiveness of the training program and on the complexity of the task. For high complexity tasks, full training is advisable for both skills acquisition and retention.
Keywords: Intra-corporeal knot tying; LASTT model; Laparoscopy; Psychomotor; Skills acquisition; Skills retention; Training.
Conflict of interest statement
CR Molinas: no conflict of interest. R Campo: no conflict of interest. Funding This study did not receive any funding and was funded by the authors’ own resources.
Figures



Similar articles
-
A randomized control trial to evaluate the importance of pre-training basic laparoscopic psychomotor skills upon the learning curve of laparoscopic intra-corporeal knot tying.Gynecol Surg. 2017;14(1):29. doi: 10.1186/s10397-017-1031-3. Epub 2017 Dec 20. Gynecol Surg. 2017. PMID: 29290752 Free PMC article.
-
Dominant hand, non-dominant hand, or both? The effect of pre-training in hand-eye coordination upon the learning curve of laparoscopic intra-corporeal knot tying.Gynecol Surg. 2017;14(1):12. doi: 10.1186/s10397-017-1015-3. Epub 2017 Jul 7. Gynecol Surg. 2017. PMID: 28890675 Free PMC article.
-
Laparoscopic simulation training: Testing for skill acquisition and retention.Surgery. 2012 Jul;152(1):12-20. doi: 10.1016/j.surg.2011.12.036. Epub 2012 Feb 16. Surgery. 2012. PMID: 22341719
-
Effect of Continuous Motion Parameter Feedback on Laparoscopic Simulation Training: A Prospective Randomized Controlled Trial on Skill Acquisition and Retention.J Surg Educ. 2018 Mar-Apr;75(2):516-526. doi: 10.1016/j.jsurg.2017.08.015. Epub 2017 Aug 31. J Surg Educ. 2018. PMID: 28864265 Clinical Trial.
-
FLS skill retention (learning) in first year surgery residents.J Surg Res. 2010 Sep;163(1):24-8. doi: 10.1016/j.jss.2010.03.057. Epub 2010 Apr 21. J Surg Res. 2010. PMID: 20605587
Cited by
-
Design and implementation of a proficiency-based, structured endoscopy course for medical students applying for a surgical specialty.Adv Med Educ Pract. 2013 May 9;4:103-15. doi: 10.2147/AMEP.S41681. Print 2013. Adv Med Educ Pract. 2013. PMID: 23901308 Free PMC article.
-
Home Surgical Skill Training Resources for Obstetrics and Gynecology Trainees During a Pandemic.Obstet Gynecol. 2020 Jul;136(1):56-64. doi: 10.1097/AOG.0000000000003931. Obstet Gynecol. 2020. PMID: 32355132 Free PMC article.
-
Comparing proficiency of obstetrics and gynaecology trainees with general surgery trainees using simulated laparoscopic tasks in Health Education England, North-West: a prospective observational study.BMJ Open. 2023 Nov 10;13(11):e075113. doi: 10.1136/bmjopen-2023-075113. BMJ Open. 2023. PMID: 37949619 Free PMC article.
-
Surgery and technical skill decay.Int J Surg. 2025 May 1;111(5):3399-3413. doi: 10.1097/JS9.0000000000002313. Int J Surg. 2025. PMID: 40085756 Free PMC article. Review.
-
A randomized control trial to evaluate the importance of pre-training basic laparoscopic psychomotor skills upon the learning curve of laparoscopic intra-corporeal knot tying.Gynecol Surg. 2017;14(1):29. doi: 10.1186/s10397-017-1031-3. Epub 2017 Dec 20. Gynecol Surg. 2017. PMID: 29290752 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources