

Results of a Medicare Bundled Payments for Care Improvement Initiative for Chronic Obstructive Pulmonary Disease Readmissions
- PMID: 28005410
- PMCID: PMC5802596
- DOI: 10.1513/AnnalsATS.201610-775BC
Results of a Medicare Bundled Payments for Care Improvement Initiative for Chronic Obstructive Pulmonary Disease Readmissions
Abstract
Rationale: Approximately 20% of Medicare beneficiaries hospitalized for acute exacerbations of chronic obstructive pulmonary disease (COPD) are readmitted within 30 days of discharge. In addition to implementing penalties for excess readmissions, the U.S. Centers for Medicare and Medicaid Services has developed Bundled Payments for Care Improvement (BPCI) initiatives to improve outcomes and control costs.
Objectives: To evaluate whether a comprehensive COPD multidisciplinary intervention focusing on inpatient, transitional, and outpatient care as part of our institution's BPCI participation would reduce 30-day all-cause readmission rates for COPD exacerbations and reduce overall costs.
Methods: We performed a pre-postintervention study comparing all-cause readmissions and costs after index hospitalization for Medicare-only patients with acute exacerbation of COPD. The primary outcome was the difference in 30-day all-cause readmission rate compared with historical control subjects; secondary outcomes included the 90-day all-cause readmission rate and also health care costs compared with BPCI target prices.
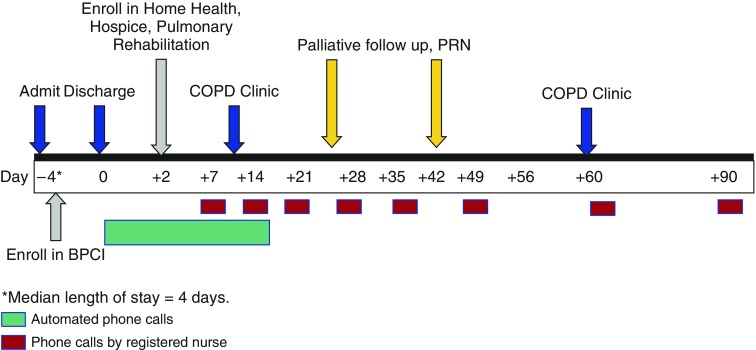
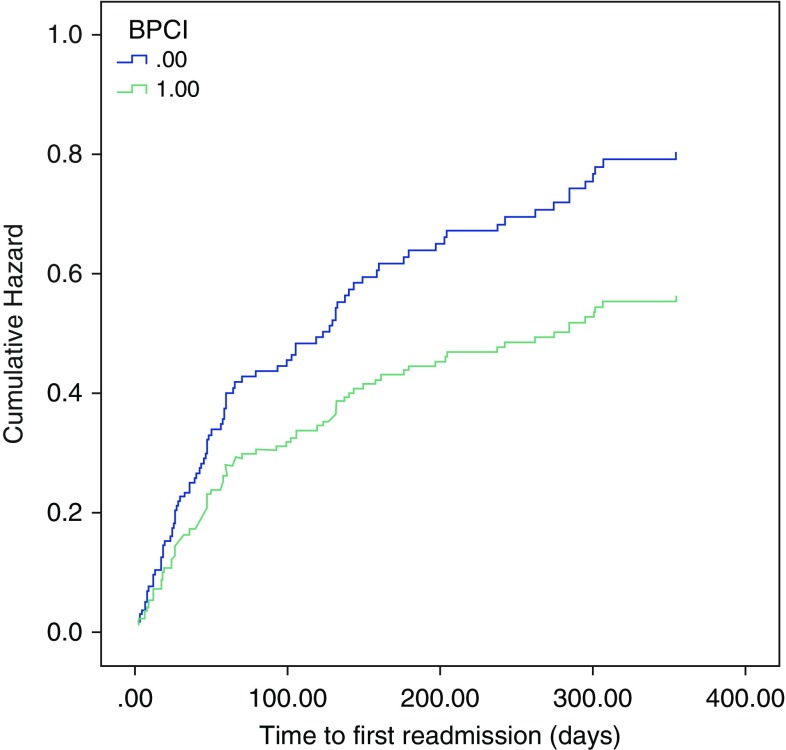
Results: Seventy-eight consecutive Medicare patients were prospectively enrolled in the BPCI intervention in 2014 and compared with 109 patients in the historical group from 2012. Patients in BPCI were more likely to receive regular follow-up phone calls, pneumococcal and influenza vaccines, home health care, durable medical equipment, and pulmonary rehabilitation, and to attend pulmonary clinic. There was no difference in all-cause readmission rates at 30 days (BPCI, 12 events [15.4%] vs. non-BPCI, 19 events [17.4%]; P = 0.711), and 90 days (21 [26.9%] vs. 37 [33.9%]; P = 0.306). Compared with BPCI target prices, we incurred 4.3% lower 90-day costs before accounting for significant investment from the health system.
Conclusions: A Medicare BPCI intervention did not reduce 30-day all-cause readmission rates or overall costs after hospitalization for acute exacerbation of COPD. Although additional studies enrolling larger numbers of patients at multiple centers may demonstrate the efficacy of our BPCI initiative for COPD readmissions, this is unlikely to be cost effective at any single center.
Keywords: bundled payment; chronic obstructive pulmonary disease; exacerbations; penalties.
Figures
Comment in
-
Medicare Bundled Payments for Care Improvement Initiative for Chronic Obstructive Pulmonary Disease Readmissions: A Negative Study That Has Positive Implications.Ann Am Thorac Soc. 2017 May;14(5):617-618. doi: 10.1513/AnnalsATS.201701-011ED. Ann Am Thorac Soc. 2017. PMID: 28459621 No abstract available.
References
-
- Centers for Medicare and Medicaid Services (CMS), Department of Health and Human Services (HHS) Medicare program; hospital inpatient prospective payment systems for acute care hospitals and the long-term care hospital prospective payment system and Fiscal Year 2014 rates; quality reporting requirements for specific providers; hospital conditions of participation; payment policies related to patient status; final rules. Fed Regist. 2013;78:50495–51040. - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–1428. - PubMed
-
- Blanchette CM, Dalal AA, Mapel D. Changes in COPD demographics and costs over 20 years. J Med Econ. 2012;15:1176–1182. - PubMed
-
- Mannino DM, Homa DM, Akinbami LJ, Ford ES, Redd SC. Chronic obstructive pulmonary disease surveillance: United States, 1971–2000. MMWR Surveill Summ. 2002;51:1–16. - PubMed
-
- Mannino DM, Braman S. The epidemiology and economics of chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2007;4:502–506. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
