

The Clinical Feasibility of Newly Developed Thin Flat-Type Bioresorbable Osteosynthesis Devices for the Internal Fixation of Zygomatic Fractures: Is There a Difference in Healing Between Bioresorbable Materials and Titanium Osteosynthesis?
- PMID: 28005767
- PMCID: PMC5110331
- DOI: 10.1097/SCS.0000000000003147
The Clinical Feasibility of Newly Developed Thin Flat-Type Bioresorbable Osteosynthesis Devices for the Internal Fixation of Zygomatic Fractures: Is There a Difference in Healing Between Bioresorbable Materials and Titanium Osteosynthesis?
Abstract
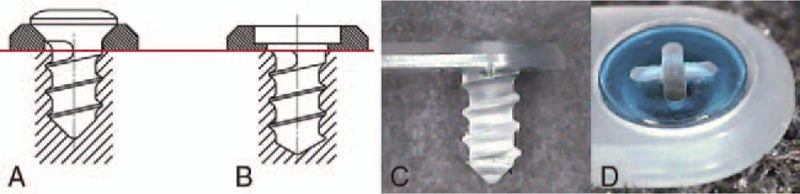
Introduction: In recent years, bioresorbable plates have undergone remarkable development. However, there has been no attendant improvement in their strength, because strength requires thickness, and complications such as palpability are related to the thickness of bioresorbable plate systems. In this clinical study, we compared the surgical management of zygomatic fractures using newly developed thinner bioresorbable materials or conventional titanium miniplates.
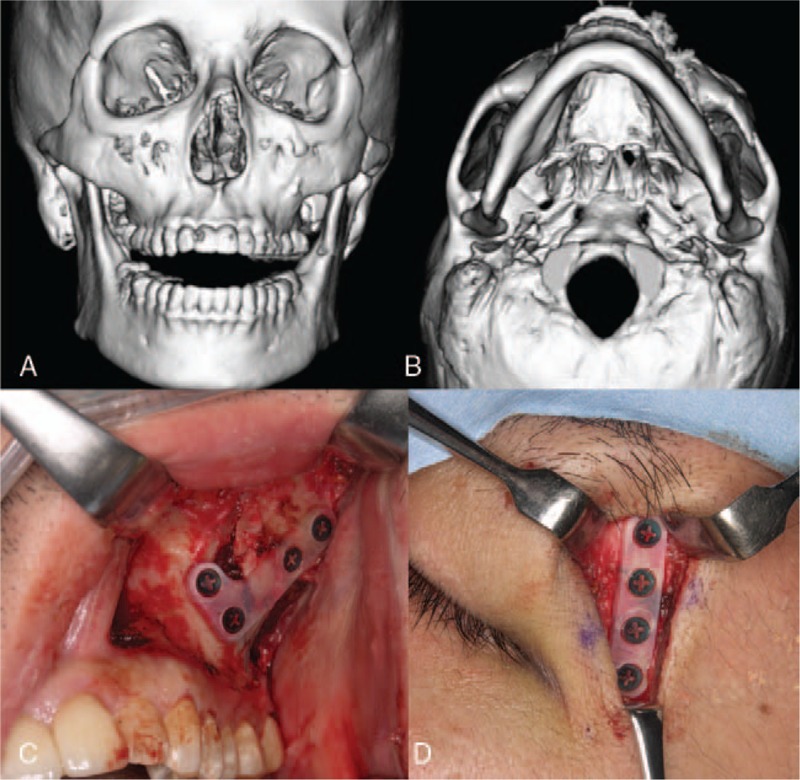
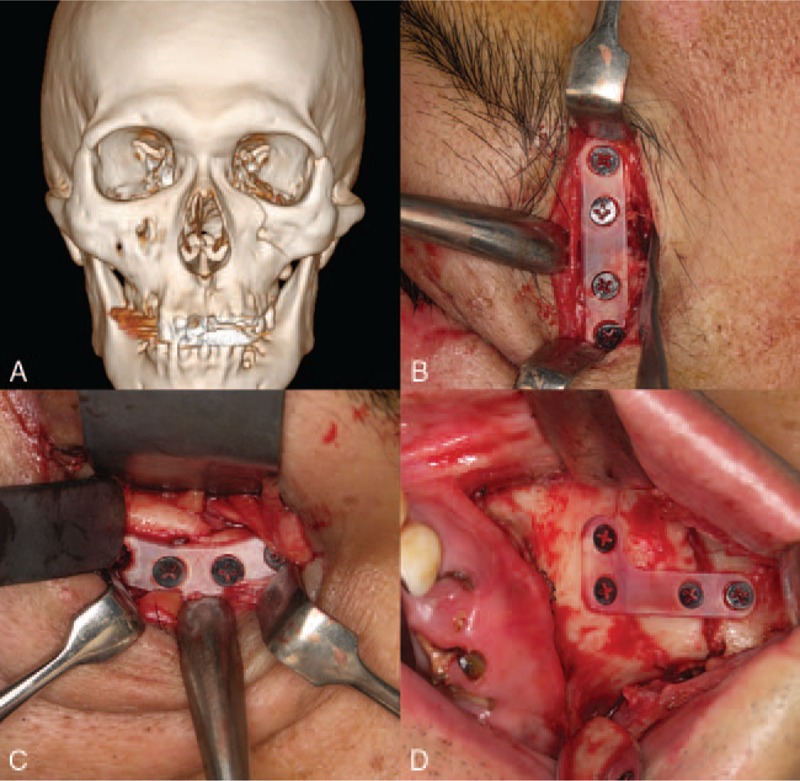
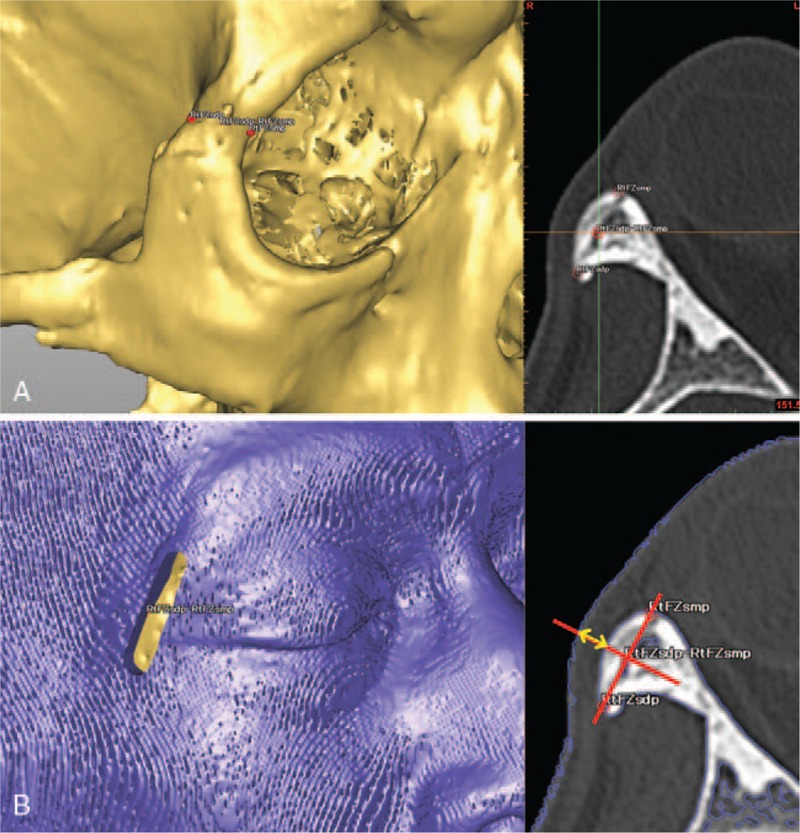
Methods: Twelve patients with zygomatic fractures were randomly divided equally into 2 groups (6 with new bioresorbable osteosynthesis materials and 6 with standard titanium miniplates). Using computed tomography, we evaluated the thickness of the soft tissue and plate at the zygomaticofrontal sutures in each patient with the help of detailed radiographic computed tomography data at 6 months postoperatively. We compared the amount of soft-tissue volume increase between the uninjured healthy and injured operated sides in each patient.
Results: Both groups eventually achieved satisfactory healing, with a favorable restoration of form and function and without any complications, including palpability. The amount of soft-tissue volume increase at the operated side relative to the uninjured healthy side using new thin bioresorbable plates was 131.1% (range: 101.5-165.8). On the other hand, that of titanium miniplates was 126.4% (range: 102.2-167.6). There was no statistically significant difference (P > 0.05).
Conclusion: This newly developed thinner flat-type bioresorbable plate system could be considered clinically useful in the treatment of zygomatic fractures even in easily palpated areas, such as the infraorbital rim or zygomaticofrontal sutures, without any healing differences in skeleton as compared with conventional titanium miniplates.
Conflict of interest statement
The authors report no conflicts of interest.
Figures

Similar articles
-
Complications after zygoma fracture fixation: is there a difference between biodegradable materials and how do they compare with titanium osteosynthesis?Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006 Apr;101(4):419-25. doi: 10.1016/j.tripleo.2005.07.026. Epub 2006 Jan 19. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006. PMID: 16545702 Clinical Trial.
-
Surgical treatment of isolated zygomatic fracture: Outcome comparison between titanium plate and bioabsorbable plate.Asian J Surg. 2018 Jul;41(4):370-376. doi: 10.1016/j.asjsur.2017.03.003. Epub 2017 May 10. Asian J Surg. 2018. PMID: 28501387
-
The sphenozygomatic suture as a key site for osteosynthesis of the orbitozygomatic complex in panfacial fractures: a biomechanical study in human cadavers based on clinical practice.Plast Reconstr Surg. 2002 Nov;110(6):1463-71; discussion 1472-5. doi: 10.1097/01.PRS.0000029360.61857.AE. Plast Reconstr Surg. 2002. PMID: 12409765
-
A comparison of combinations of titanium and resorbable plating systems for repair of isolated zygomatic fractures in the adult: a quantitative biomechanical study.Ann Plast Surg. 2005 Apr;54(4):402-8. doi: 10.1097/01.sap.0000151484.59846.62. Ann Plast Surg. 2005. PMID: 15785282 Review.
-
A biomechanical analysis of the orbital zygomatic complex in human cadavers: examination of load sharing and failure patterns after fixation with titanium and bioresorbable systems.J Craniofac Surg. 1999 Sep;10(5):400-3. doi: 10.1097/00001665-199909000-00005. J Craniofac Surg. 1999. PMID: 10726510 Review. No abstract available.
Cited by
-
Complications of Poly-l-Lactic Acid and Polyglycolic Acid (PLLA/PGA) Osteosynthesis Systems for Maxillofacial Surgery: A Retrospective Clinical Investigation.Polymers (Basel). 2021 Mar 14;13(6):889. doi: 10.3390/polym13060889. Polymers (Basel). 2021. PMID: 33799342 Free PMC article.
-
Efficacy of bioresorbable plates in the osteosynthesis of linear mandibular fractures.Natl J Maxillofac Surg. 2020 Jan-Jun;11(1):98-105. doi: 10.4103/njms.NJMS_54_19. Epub 2020 Jun 18. Natl J Maxillofac Surg. 2020. PMID: 33041585 Free PMC article.
-
Biomechanical Loading Comparison between Titanium and Unsintered Hydroxyapatite/Poly-L-Lactide Plate System for Fixation of Mandibular Subcondylar Fractures.Materials (Basel). 2019 May 13;12(9):1557. doi: 10.3390/ma12091557. Materials (Basel). 2019. PMID: 31085981 Free PMC article.
-
Biocompatible Materials in Otorhinolaryngology and Their Antibacterial Properties.Int J Mol Sci. 2022 Feb 25;23(5):2575. doi: 10.3390/ijms23052575. Int J Mol Sci. 2022. PMID: 35269718 Free PMC article. Review.
-
In Silico Biomechanical Evaluation of WE43 Magnesium Plates for Mandibular Fracture Fixation.Front Bioeng Biotechnol. 2022 Feb 10;9:803103. doi: 10.3389/fbioe.2021.803103. eCollection 2021. Front Bioeng Biotechnol. 2022. PMID: 35223813 Free PMC article.
References
-
- Enislidis G, Pichorner S, Lambert F, et al. Fixation of zygomatic fractures with a new bioresorbable copolymer osteosynthesis system. Preliminary results. Int J Oral Maxillofac Surg 1998; 27:352–355. - PubMed
-
- Eppley BL, Sadove MA. Effects of resorbable fixation on craniofacial growth: a pilot experimental study. J Craniomaxillofac Surg 1992; 3:190–196. - PubMed
-
- Eppley BL. Resorbable biotechnology for craniomaxillofacial surgery. J Craniofac Surg 1997; 2:85–86. - PubMed
-
- Suuronen R, Haers PE, Lindqvist C, et al. Update on bioresorbable plates in maxillofacial surgery. Facial Plast Surg 1999; 15:61–72. - PubMed
-
- Yerit KC, Enislidis G, Schopper C, et al. Fixation of mandibular fractures with bioresorbable plates and screws. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002; 94:294–300. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
