

Benchmarking Prehospital and Emergency Department Care for Argentine Children with Traumatic Brain Injury: For the South American Guideline Adherence Group
- PMID: 28005912
- PMCID: PMC5179077
- DOI: 10.1371/journal.pone.0166478
Benchmarking Prehospital and Emergency Department Care for Argentine Children with Traumatic Brain Injury: For the South American Guideline Adherence Group
Abstract
Objective: There is little information on the type of early care provided to children with traumatic brain injury (TBI) in low middle income countries. We benchmarked early prehospital [PH] and emergency department [ED] pediatric TBI care in Argentina.
Methods: We conducted a secondary analysis of data from patients previously enrolled in a prospective seven center study of children with TBI. Eligible participants were patients 0-18 years, and had diagnosis of TBI (admission Glasgow Coma scale score [GCS] < 13 or with GCS 14-15 and abnormal head CT scan within 48 hours of admission, and head AIS > 0). Outcomes were transport type, transport time, PH and ED adherence to best practice, and discharge Pediatric Cerebral Performance Category Scale (PCPC) and Pediatric Overall Performance category Scale (POPC).
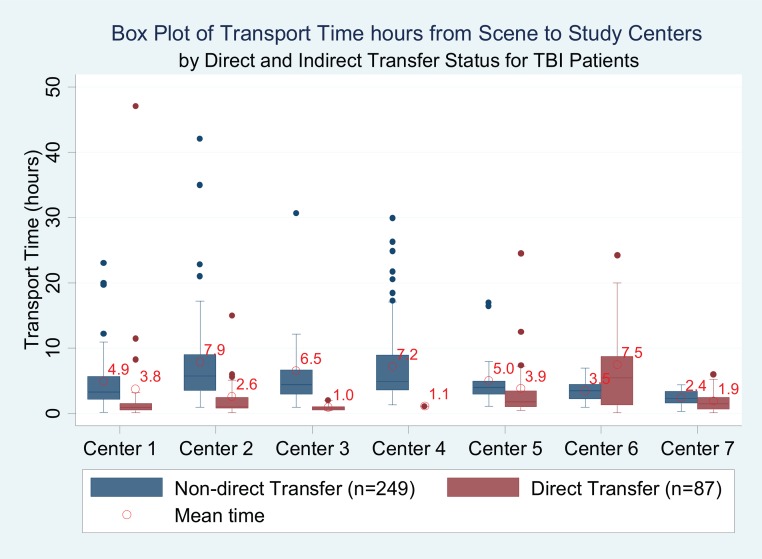
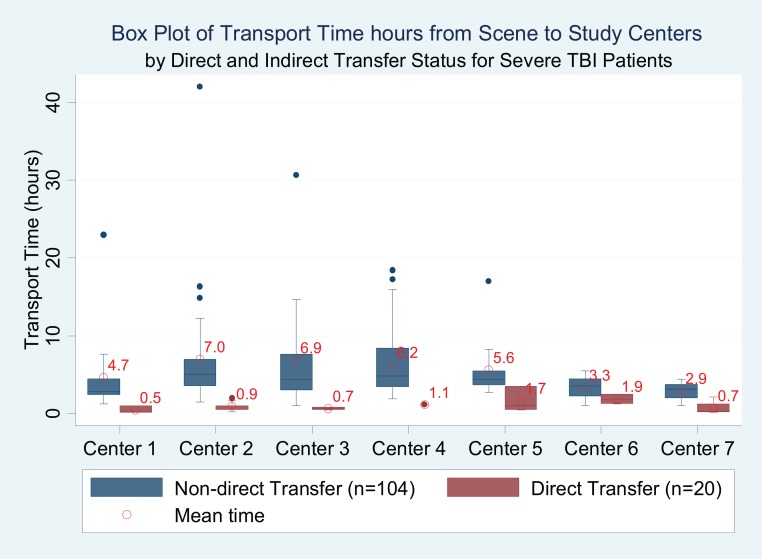
Results: Of the 366 children, mean age was 8.7 (5.0) years, 58% were male, 90% had isolated TBI and 45.4% were transported by private vehicle. 50 (34.7%) of the 144 children with severe TBI (39.3% of all TBI patients) were transported by private vehicle. Most (267; 73%) patients received initial TBI care at an index hospital prior to study center admission, including children with severe (81.9%) TBI. Transport times were shorter for those patients who were directly transported by ambulance to study center than for the whole cohort (1.4 vs.5.5 hours). Ambulance blood pressure data were recorded in 30.9%. ED guideline adherence rate was higher than PH guideline adherence rate (84.8% vs. 26.4%). For patients directly transferred from scene to study trauma centers, longer transport time was associated with worse discharge outcome (PCPC aOR 1.10 [1.04, 1.18] and (POPC aOR 1.10 [1.04, 1.18]). There was no relationship between PH or ED TBI guideline adherence rate and discharge POPC and PCPC.
Conclusion: This study benchmarks early pediatric TBI care in Argentina and shows that many critically injured children with TBI do not receive timely or best practice PH care, that PH guideline adherence rate is low and that longer transport time was associated with poor discharge outcomes for patients with direct transfer status. There is an urgent need to improve the early care of children with TBI in Argentina, especially timely transportation to a hospital.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization. Violence and Injury Prevention: Injuries and Violence: The Facts (2015) http://www.who.int/violence_injury_prevention/key_facts/en/ Accessed August 3, 2015.
-
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet, 385 (2015), pp. 117–171. 10.1016/S0140-6736(14)61682-2 - DOI - PMC - PubMed
-
- Hyder AA, Wunderlich CA, Puvanachandra P, Gururaj G, Kobusingye OC. The impact of traumatic brain injuries: a global perspective. NeuroRehabilitation. 2007; 22: 341–353. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
