

Neutrophil-to-lymphocyte ratio correlates with proinflammatory neutrophils and predicts death in low model for end-stage liver disease patients with cirrhosis
- PMID: 28006875
- PMCID: PMC5529041
- DOI: 10.1002/lt.24702
Neutrophil-to-lymphocyte ratio correlates with proinflammatory neutrophils and predicts death in low model for end-stage liver disease patients with cirrhosis
Abstract
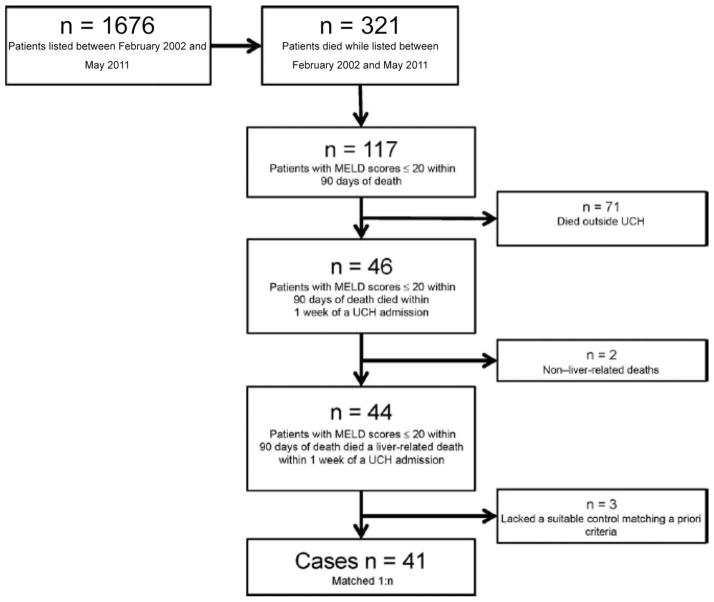
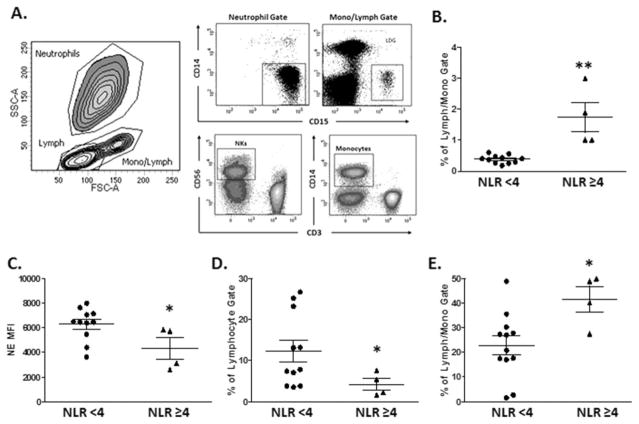
The Model for End-Stage Liver Disease (MELD) score has reduced accuracy for liver transplantation (LT) wait-list mortality when MELD ≤ 20. Neutrophil-to-lymphocyte ratio (NLR) is a biomarker associated with systemic inflammation and may predict cirrhotic decompensation and death. We aimed to evaluate the prognostic utility of high NLR (≥4) for liver-related death among low MELD patients listed for LT, controlling for stage of cirrhosis. In a nested case-control study of cirrhotic adults awaiting LT (February 2002 to May 2011), cases were LT candidates with a liver-related death and MELD ≤ 20 within 90 days of death. Controls were similar LT candidates who were alive for ≥90 days after LT listing. NLR and other covariates were assessed at the date of lowest MELD, within 90 days of death for cases and within 90 days after listing for controls. There were 41 cases and 66 controls; MELD scores were similar. NLR 25th, 50th, 75th percentile cutoffs were 1.9, 3.1, and 6.8. NLR was ≥ 4 in 25/41 (61%) cases and in 17/66 (26%) controls. In univariate analysis, NLR (continuous ≥ 1.9, ≥ 4, ≥ 6.8), increasing cirrhosis stage, jaundice, encephalopathy, serum sodium, and albumin and nonselective beta-blocker use were significantly (P < 0.01) associated with liver-related death. In multivariate analysis, NLR of ≥1.9, ≥ 4, ≥ 6.8 were each associated with liver-related death. Furthermore, we found that NLR correlated with the frequency of circulating low-density granulocytes, previously identified as displaying proinflammatory properties, as well as monocytes. In conclusion, elevated NLR is associated with liver-related death, independent of MELD and cirrhosis stage. High NLR may aid in determining risk for cirrhotic decompensation, need for increased monitoring, and urgency for expedited LT in candidates with low MELD. Liver Transplantation 23 155-165 2017 AASLD.
© 2016 by the American Association for the Study of Liver Diseases.
Figures
Similar articles
-
MELD scores with incorporation of serum sodium and death prediction in cirrhotic patients on the waiting list for liver transplantation: a single center experience in southern Brazil.Clin Transplant. 2012 Jul-Aug;26(4):E395-401. doi: 10.1111/j.1399-0012.2012.01688.x. Clin Transplant. 2012. PMID: 22882694 Clinical Trial.
-
Stage of cirrhosis predicts the risk of liver-related death in patients with low Model for End-Stage Liver Disease scores and cirrhosis awaiting liver transplantation.Liver Transpl. 2014 Oct;20(10):1193-201. doi: 10.1002/lt.23929. Epub 2014 Aug 26. Liver Transpl. 2014. PMID: 24916539 Free PMC article.
-
Disability in patients with end-stage liver disease: Results from the functional assessment in liver transplantation study.Liver Transpl. 2017 Mar;23(3):292-298. doi: 10.1002/lt.24684. Liver Transpl. 2017. PMID: 27884053 Free PMC article.
-
Model for end-stage liver disease and organ allocation in liver transplantation: where are we and where should we go?J Chin Med Assoc. 2006 May;69(5):193-8. doi: 10.1016/S1726-4901(09)70217-5. J Chin Med Assoc. 2006. PMID: 16835979 Review.
-
MELD 3.0 in Advanced Chronic Liver Disease.Annu Rev Med. 2024 Jan 29;75:233-245. doi: 10.1146/annurev-med-051322-122539. Epub 2023 Sep 26. Annu Rev Med. 2024. PMID: 37751367 Review.
Cited by
-
Neutrophil percentage-to-albumin ratio as predictor for mortality in patients undergoing endoscopic intervention for variceal hemorrhage.Eur J Med Res. 2025 Apr 26;30(1):329. doi: 10.1186/s40001-025-02489-4. Eur J Med Res. 2025. PMID: 40281590 Free PMC article.
-
Baseline Neutrophil-to-Lymphocyte Ratio Is Independently Associated With 90-Day Transplant-Free Mortality in Patients With Cirrhosis.Front Med (Lausanne). 2021 Aug 31;8:726950. doi: 10.3389/fmed.2021.726950. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34532334 Free PMC article.
-
Neutrophils: tissue and circulating signatures of pediatric non-alcoholic fatty liver disease.Front Cell Dev Biol. 2024 Jan 4;11:1336033. doi: 10.3389/fcell.2023.1336033. eCollection 2023. Front Cell Dev Biol. 2024. PMID: 38239291 Free PMC article. Review.
-
Risk stratification for early bacteremia after living donor liver transplantation: a retrospective observational cohort study.BMC Surg. 2020 Mar 12;20(1):2. doi: 10.1186/s12893-019-0658-6. BMC Surg. 2020. PMID: 32160890 Free PMC article.
-
Neutrophil to lymphocyte ratio and albumin bilirubin grade in hepatocellular carcinoma: A systematic review.World J Gastroenterol. 2020 Sep 7;26(33):5022-5049. doi: 10.3748/wjg.v26.i33.5022. World J Gastroenterol. 2020. PMID: 32952347 Free PMC article.
References
-
- Said A, Williams J, Holden J, Remington P, Gangnon R, Musat A, Lucey MR. Model for End-Stage Liver Disease score predicts mortality across a broad spectrum of liver disease. J Hepatol. 2004;40:897–903. - PubMed
-
- Wiesner R, Edwards E, Freeman R, Harper A, Kim R, Kamath P, et al. for United Network for Organ Sharing Liver Disease Severity Score Committee. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology. 2003;124:91–96. - PubMed
-
- Kamath PS, Wiesner RH, Malinchoc M, Kremers W, Therneau TM, Kosberg CL, et al. A model to predict survival in patients with end-stage liver disease. Hepatology. 2001;33:464–470. - PubMed
-
- Freeman RB, Wiesner RH, Edwards E, Harper A, Merion R, Wolfe R for United Network for Organ Sharing Organ Procurement and Transplantation Network Liver and Transplantation Committee. Results of the first year of the new liver allocation plan. Liver Transpl. 2004;10:7–15. - PubMed
-
- Biggins SW, Bambha K. MELD-based liver allocation: who is underserved? Semin Liver Dis. 2006;26:211–220. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
