

Genomic landscape of colorectal cancer in Japan: clinical implications of comprehensive genomic sequencing for precision medicine
- PMID: 28007036
- PMCID: PMC5180401
- DOI: 10.1186/s13073-016-0387-8
Genomic landscape of colorectal cancer in Japan: clinical implications of comprehensive genomic sequencing for precision medicine
Abstract
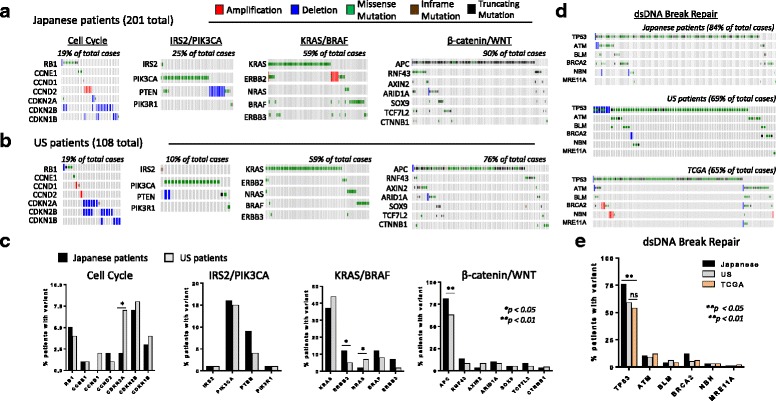
Background: Comprehensive genomic sequencing (CGS) has the potential to revolutionize precision medicine for cancer patients across the globe. However, to date large-scale genomic sequencing of cancer patients has been limited to Western populations. In order to understand possible ethnic and geographic differences and to explore the broader application of CGS to other populations, we sequenced a panel of 415 important cancer genes to characterize clinically actionable genomic driver events in 201 Japanese patients with colorectal cancer (CRC).
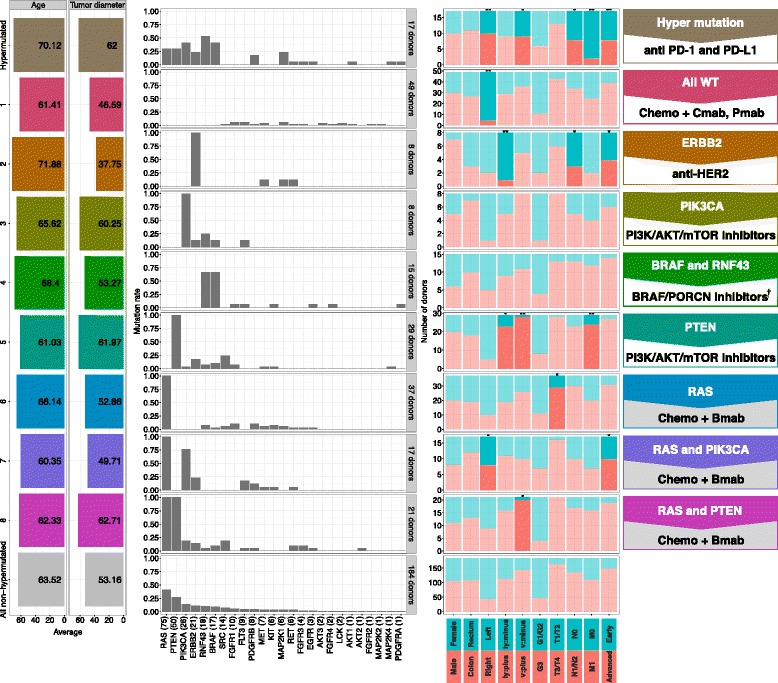
Methods: Using next-generation sequencing methods, we examined all exons of 415 known cancer genes in Japanese CRC patients (n = 201) and evaluated for concordance among independent data obtained from US patients with CRC (n = 108) and from The Cancer Genome Atlas-CRC whole exome sequencing (WES) database (n = 224). Mutation data from non-hypermutated Japanese CRC patients were extracted and clustered by gene mutation patterns. Two different sets of genes from the 415-gene panel were used for clustering: 61 genes with frequent alteration in CRC and 26 genes that are clinically actionable in CRC.
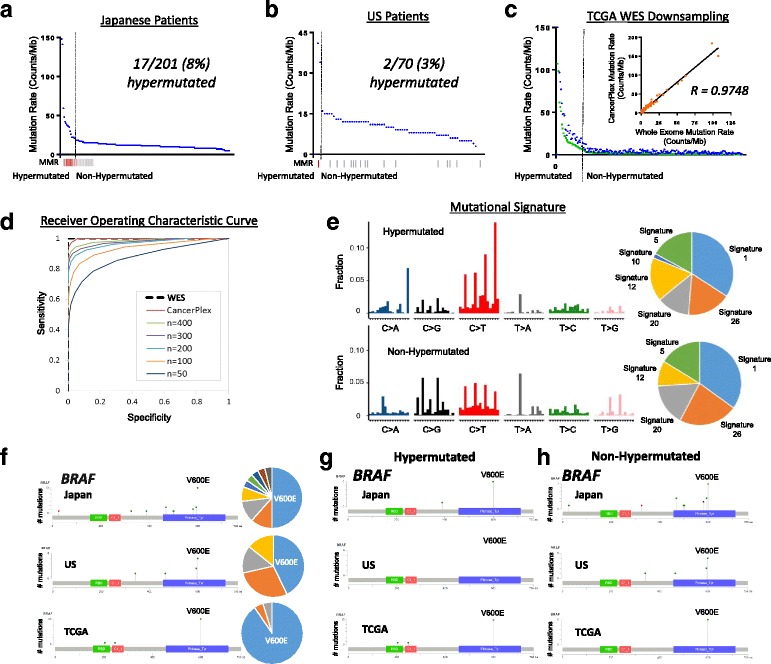
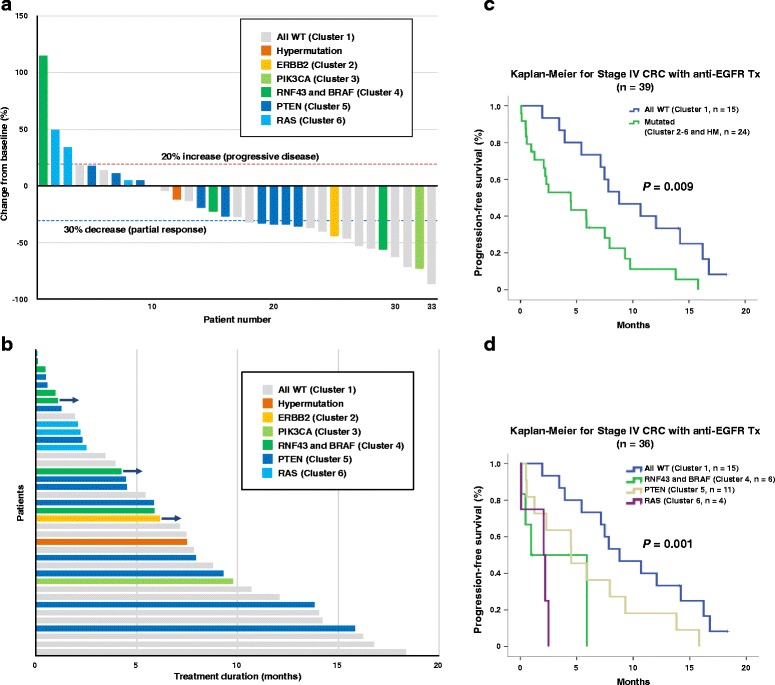
Results: The 415-gene panel is able to identify all of the critical mutations in tumor samples as well as WES, including identifying hypermutated tumors. Although the overall mutation spectrum of the Japanese patients is similar to that of the Western population, we found significant differences in the frequencies of mutations in ERBB2 and BRAF. We show that the 415-gene panel identifies a number of clinically actionable mutations in KRAS, NRAS, and BRAF that are not detected by hot-spot testing. We also discovered that 26% of cases have mutations in genes involved in DNA double-strand break repair pathway. Unsupervised clustering revealed that a panel of 26 genes can be used to classify the patients into eight different categories, each of which can optimally be treated with a particular combination therapy.
Conclusions: Use of a panel of 415 genes can reliably identify all of the critical mutations in CRC patients and this information of CGS can be used to determine the most optimal treatment for patients of all ethnicities.
Keywords: Actionable driver mutation; Colorectal cancer; Comprehensive genomic sequencing; Ethnicity; Hypermutation; Japanese; Precision medicine.
Figures
Similar articles
-
Next generation sequencing-based gene panel tests for the management of solid tumors.Cancer Sci. 2019 Jan;110(1):6-15. doi: 10.1111/cas.13837. Epub 2018 Nov 27. Cancer Sci. 2019. PMID: 30338623 Free PMC article. Review.
-
Performance of Next-Generation Sequencing for the Detection of Microsatellite Instability in Colorectal Cancer With Deficient DNA Mismatch Repair.Gastroenterology. 2021 Sep;161(3):814-826.e7. doi: 10.1053/j.gastro.2021.05.007. Epub 2021 May 13. Gastroenterology. 2021. PMID: 33992635
-
Comparison of TCGA and GENIE genomic datasets for the detection of clinically actionable alterations in breast cancer.Sci Rep. 2019 Feb 6;9(1):1482. doi: 10.1038/s41598-018-37574-8. Sci Rep. 2019. PMID: 30728399 Free PMC article.
-
Genomic Signature of Driver Genes Identified by Target Next-Generation Sequencing in Chinese Non-Small Cell Lung Cancer.Oncologist. 2019 Nov;24(11):e1070-e1081. doi: 10.1634/theoncologist.2018-0572. Epub 2019 Mar 22. Oncologist. 2019. PMID: 30902917 Free PMC article.
-
Actionable Potentials of Less Frequently Mutated Genes in Colorectal Cancer and Their Roles in Precision Medicine.Biomolecules. 2020 Mar 20;10(3):476. doi: 10.3390/biom10030476. Biomolecules. 2020. PMID: 32245111 Free PMC article. Review.
Cited by
-
Identifying Optimal Loci for the Molecular Diagnosis of Microsatellite Instability.Clin Chem. 2020 Oct 1;66(10):1310-1318. doi: 10.1093/clinchem/hvaa177. Clin Chem. 2020. PMID: 33001187 Free PMC article.
-
Precision medicine for gastrointestinal cancer: Recent progress and future perspective.World J Gastrointest Oncol. 2020 Jan 15;12(1):1-20. doi: 10.4251/wjgo.v12.i1.1. World J Gastrointest Oncol. 2020. PMID: 31966910 Free PMC article. Review.
-
Genomic and transcriptomic analysis of Korean colorectal cancer patients.Genes Genomics. 2022 Aug;44(8):967-979. doi: 10.1007/s13258-022-01275-4. Epub 2022 Jun 25. Genes Genomics. 2022. PMID: 35751785 Free PMC article.
-
Profiling of host genetic alterations and intra-tumor microbiomes in colorectal cancer.Comput Struct Biotechnol J. 2021 Jun 4;19:3330-3338. doi: 10.1016/j.csbj.2021.05.049. eCollection 2021. Comput Struct Biotechnol J. 2021. PMID: 34188781 Free PMC article.
-
Next generation sequencing-based gene panel tests for the management of solid tumors.Cancer Sci. 2019 Jan;110(1):6-15. doi: 10.1111/cas.13837. Epub 2018 Nov 27. Cancer Sci. 2019. PMID: 30338623 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
