

High-Sensitivity Cardiac Troponin, Statin Therapy, and Risk of Coronary Heart Disease
- PMID: 28007133
- PMCID: PMC5176330
- DOI: 10.1016/j.jacc.2016.10.020
High-Sensitivity Cardiac Troponin, Statin Therapy, and Risk of Coronary Heart Disease
Abstract
Background: Cardiac troponin is an independent predictor of cardiovascular mortality in individuals without symptoms or signs of cardiovascular disease. The mechanisms for this association are uncertain, and a role for troponin testing in the prevention of coronary heart disease has yet to be established.
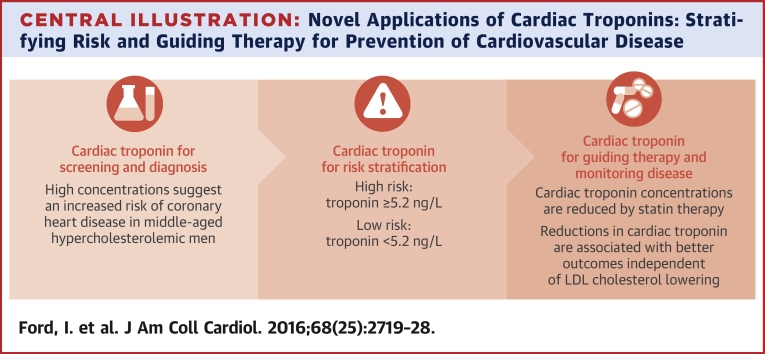
Objectives: This study sought to determine whether troponin concentration could predict coronary events, be modified by statins, and reflect response to therapy in a primary prevention population.
Methods: WOSCOPS (West of Scotland Coronary Prevention Study) randomized men with raised low-density lipoprotein cholesterol and no history of myocardial infarction to pravastatin 40 mg once daily or placebo for 5 years. Plasma cardiac troponin I concentration was measured with a high-sensitivity assay at baseline and at 1 year in 3,318 participants.
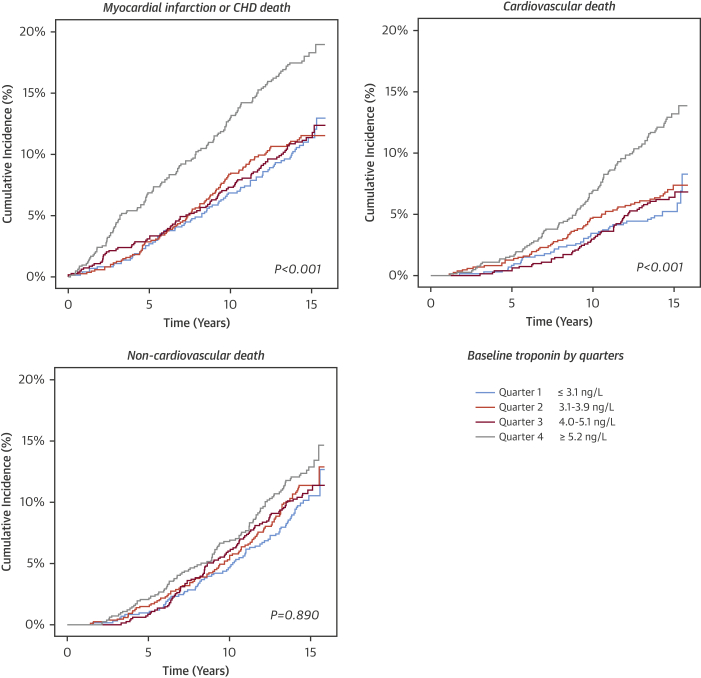
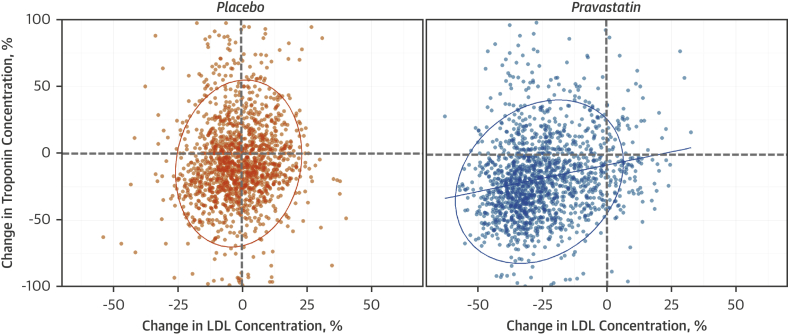
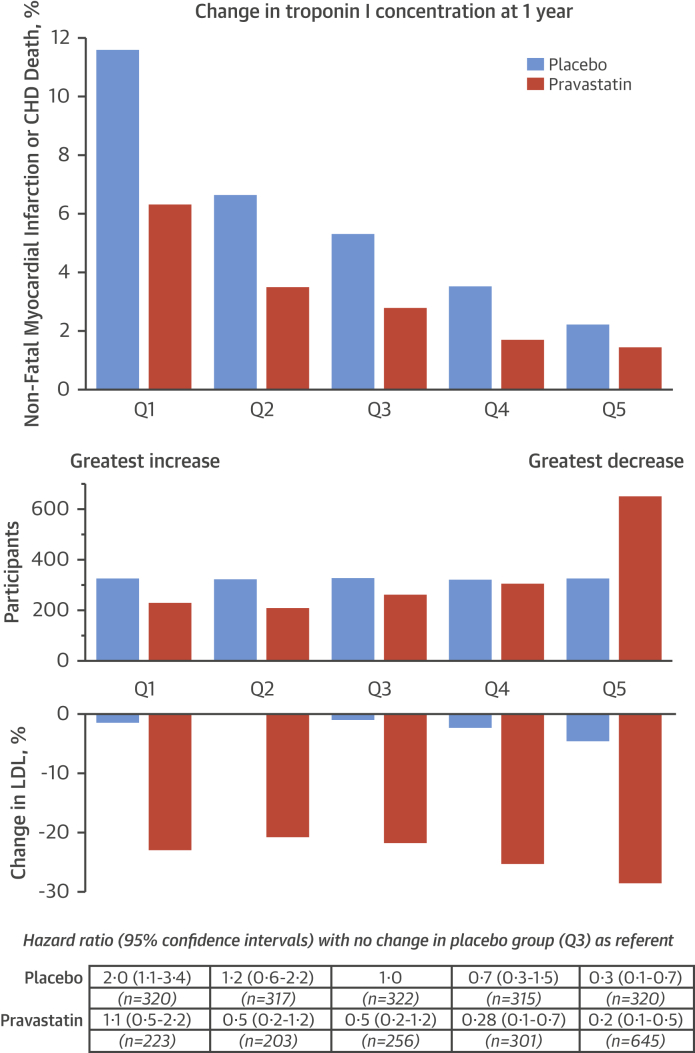
Results: Baseline troponin was an independent predictor of myocardial infarction or death from coronary heart disease (hazard ratio [HR]: 2.3; 95% confidence interval [CI]: 1.4 to 3.7) for the highest (≥5.2 ng/l) versus lowest (≤3.1 ng/l) quarter of troponin (p < 0.001). There was a 5-fold greater reduction in coronary events when troponin concentrations decreased by more than a quarter, rather than increased by more than a quarter, for both placebo (HR: 0.29; 95% CI: 0.12 to 0.72 vs. HR: 1.95; 95% CI: 1.09 to 3.49; p < 0.001 for trend) and pravastatin (HR: 0.23; 95% CI: 0.10 to 0.53 vs. HR: 1.08; 95% CI: 0.53 to 2.21; p < 0.001 for trend). Pravastatin reduced troponin concentration by 13% (10% to 15%; placebo adjusted, p < 0.001) and doubled the number of men whose troponin fell more than a quarter (p < 0.001), which identified them as having the lowest risk for future coronary events (1.4% over 5 years).
Conclusions: Troponin concentration predicts coronary events, is reduced by statin therapy, and change at 1 year is associated with future coronary risk independent of cholesterol lowering. Serial troponin measurements have major potential to assess cardiovascular risk and monitor the impact of therapeutic interventions.
Keywords: cardiac troponin; cardiovascular risk; primary prevention; statins.
Copyright © 2016 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
High-Sensitivity Cardiac Troponin and Primary Prevention: An Important New Role.J Am Coll Cardiol. 2016 Dec 27;68(25):2729-2732. doi: 10.1016/j.jacc.2016.11.006. J Am Coll Cardiol. 2016. PMID: 28007134 No abstract available.
-
Concerns About the Stability of hsTnI Assay After 20 Years of Storage.J Am Coll Cardiol. 2017 Jun 6;69(22):2772-2773. doi: 10.1016/j.jacc.2017.01.077. J Am Coll Cardiol. 2017. PMID: 28571645 No abstract available.
-
Relativism and Low-Density Lipoprotein Cholesterol: Absolute or Relative Truth?J Am Coll Cardiol. 2017 Jun 6;69(22):2773-2774. doi: 10.1016/j.jacc.2017.01.076. J Am Coll Cardiol. 2017. PMID: 28571646 No abstract available.
References
-
- Shepherd J., Cobbe S.M., Ford I. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. N Engl J Med. 1995;333:1301–1307. - PubMed
-
- Ford I., Murray H., Packard C.J., Shepherd J., Macfarlane P.W., Cobbe S.M. Long-term follow-up of the West of Scotland Coronary Prevention Study. N Engl J Med. 2007;357:1477–1486. - PubMed
-
- Downs J.R., Clearfield M., Weis S. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS: Air Force/Texas Coronary Atherosclerosis Prevention Study. JAMA. 1998;279:1615–1622. - PubMed
-
- Ridker P.M., Danielson E., Fonseca F.A. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008;359:2195–2207. - PubMed
-
- Redberg R.F., Katz M.H. Healthy men should not take statins. JAMA. 2012;307:1491–1492. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
