

Second line drug susceptibility testing to inform the treatment of rifampin-resistant tuberculosis: a quantitative perspective
- PMID: 28007660
- PMCID: PMC5576040
- DOI: 10.1016/j.ijid.2016.12.010
Second line drug susceptibility testing to inform the treatment of rifampin-resistant tuberculosis: a quantitative perspective
Abstract
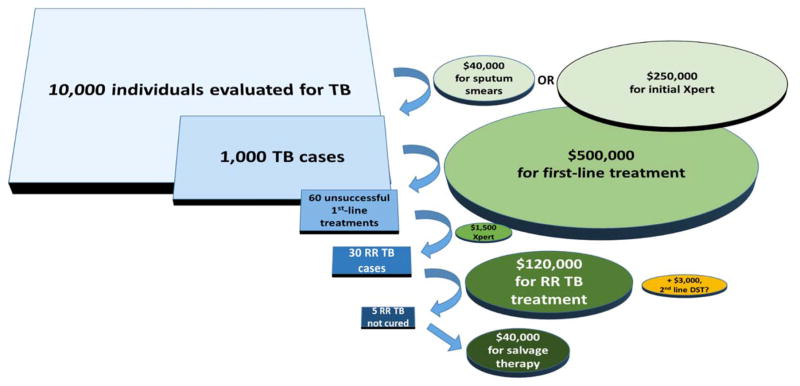
Treatment failure and resistance amplification are common among patients with rifampin-resistant tuberculosis (TB). Drug susceptibility testing (DST) for second-line drugs is recommended for these patients, but logistical difficulties have impeded widespread implementation of second-line DST in many settings. To provide a quantitative perspective on the decision to scale up second-line DST, we synthesize literature on the prevalence of second-line drug resistance, the expected clinical and epidemiologic benefits of using second-line DST to ensure that patients with rifampin-resistant TB receive effective regimens, and the costs of implementing (or not implementing) second-line DST for all individuals diagnosed with rifampin-resistant TB. We conclude that, in most settings, second-line DST could substantially improve treatment outcomes for patients with rifampin-resistant TB, reduce transmission of drug-resistant TB, prevent amplification of drug resistance, and be affordable or even cost-saving. Given the large investment made in each patient treated for rifampin-resistant TB, these payoffs would come at relatively small incremental cost. These anticipated benefits likely justify addressing the real challenges faced in implementing second-line DST in most high-burden settings.
Keywords: Cost effectiveness; Diagnostics; Drug resistance; Regimen selection; Treatment outcomes.
Copyright © 2016 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Figures
References
-
- Global Tuberculosis Report 2016 [Internet] Geneva: World Health Organization; 2016. [cited 2016 Oct 27]. Available from: http://www.who.int/tb/publications/global_report/en/
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
