

Stroke outcomes are worse with larger leukoaraiosis volumes
- PMID: 28008000
- PMCID: PMC6276917
- DOI: 10.1093/brain/aww259
Stroke outcomes are worse with larger leukoaraiosis volumes
Abstract
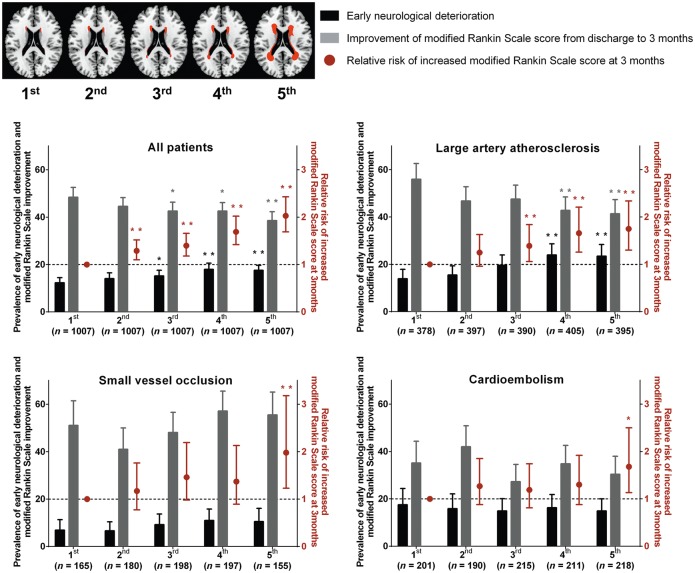
Leukoaraiosis or white matter hyperintensities are frequently observed on magnetic resonance imaging of stroke patients. We investigated how white matter hyperintensity volumes affect stroke outcomes, generally and by subtype. In total, 5035 acute ischaemic stroke patients were enrolled. Strokes were classified as large artery atherosclerosis, small vessel occlusion, or cardioembolism. White matter hyperintensity volumes were stratified into quintiles. Mean age (± standard deviation) was 66.3 ± 12.8, 59.6% male. Median (interquartile range) modified Rankin Scale score was 2 (1-3) at discharge and 1 (0-3) at 3 months; 16.5% experienced early neurological deterioration, and 3.3% recurrent stroke. The Cochran-Mantel-Haenszel test with adjustment for age, stroke severity, sex, and thrombolysis status showed that the distributions of 3-month modified Rankin Scale scores differed across white matter hyperintensity quintiles (P < 0.001). Multiple ordinal logistic regression analysis showed that higher white matter hyperintensity quintiles were independently associated with worse 3-month modified Rankin Scale scores; adjusted odds ratios (95% confidence interval) for the second to fifth quintiles versus the first quintile were 1.29 (1.10-1.52), 1.40 (1.18-1.66), 1.69 (1.42-2.02) and 2.03 (1.69-2.43), respectively. For large artery atherosclerosis (39.0%), outcomes varied by white matter hyperintensity volume (P = 0.01, Cochran-Mantel-Haenszel test), and the upper three white matter hyperintensity quintiles (versus the first quintile) had worse 3-month modified Rankin Scale scores; adjusted odds ratios were 1.45 (1.10-1.90), 1.86 (1.41-2.47), and 1.89 (1.41-2.54), respectively. Patients with large artery atherosclerosis were vulnerable to early neurological deterioration (19.4%), and the top two white matter hyperintensity quintiles were more vulnerable still: 23.5% and 22.3%. Moreover, higher white matter hyperintensities were associated with poor modified Rankin Scale improvement: adjusted odds ratios for the upper two quintiles versus the first quintile were 0.66 (0.47-0.94) and 0.62 (0.43-0.89), respectively. For small vessel occlusion (17.8%), outcomes tended to vary by white matter hyperintensitiy volume (P = 0.10, Cochran-Mantel-Haenszel test), and the highest quintile was associated with worse 3-month modified Rankin Scale scores: adjusted odds ratio for the fifth quintile versus first quintile, 1.98 (1.23-3.18). In this subtype, worse white matter hyperintensities were associated with worse National Institute of Health Stroke Scale scores at presentation. For cardioembolism (20.6%), outcomes did not vary significantly by white matter hyperintensity volume (P = 0.19, Cochran-Mantel-Haenszel test); however, the adjusted odds ratio for the highest versus lowest quintiles was 1.62 (1.09-2.40). Regardless of stroke subtype, white matter hyperintensities were not associated with stroke recurrence within 3 months of follow-up. In conclusion, white matter hyperintensity volume independently correlates with stroke outcomes in acute ischaemic stroke. There are some suggestions that stroke outcomes may be affected by leukoaraiosis differentially depending on stroke subtypes, to be confirmed in future investigations.
Keywords: ischaemic stroke; magnetic resonance image; outcome; white matter hyperintensities.
© The Author (2016). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Adams HP Jr Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, et al.Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993; 24: 35–41. - PubMed
-
- Aries MJ, Uyttenboogaart M, Vroomen PC, De Keyser J, Luijckx GJ. tPA treatment for acute ischaemic stroke in patients with leukoaraiosis. Eur J Neurol 2010; 17: 866–70. - PubMed
-
- Ay H, Arsava EM, Rosand J, Furie KL, Singhal AB, Schaefer PW, et al.Severity of leukoaraiosis and susceptibility to infarct growth in acute stroke. Stroke 2008; 39: 1409–13. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
