

Communication practices and awareness of resources for acromegaly patients among endocrinologists
- PMID: 28008238
- PMCID: PMC5167300
- DOI: 10.2147/PPA.S119570
Communication practices and awareness of resources for acromegaly patients among endocrinologists
Abstract
Purpose: This study was designed to assess the awareness and utilization of resources to improve patients' treatment experiences among endocrinologists who currently treat patients with acromegaly.
Methods: A total of 4,280 US endocrinologists were randomly selected from the CMS National Plan and Provider Enumeration System and were invited by mail to participate in a 20-minute online survey. In order to qualify, respondents had to be the primary physician making treatment decisions for at least one patient for their acromegaly.
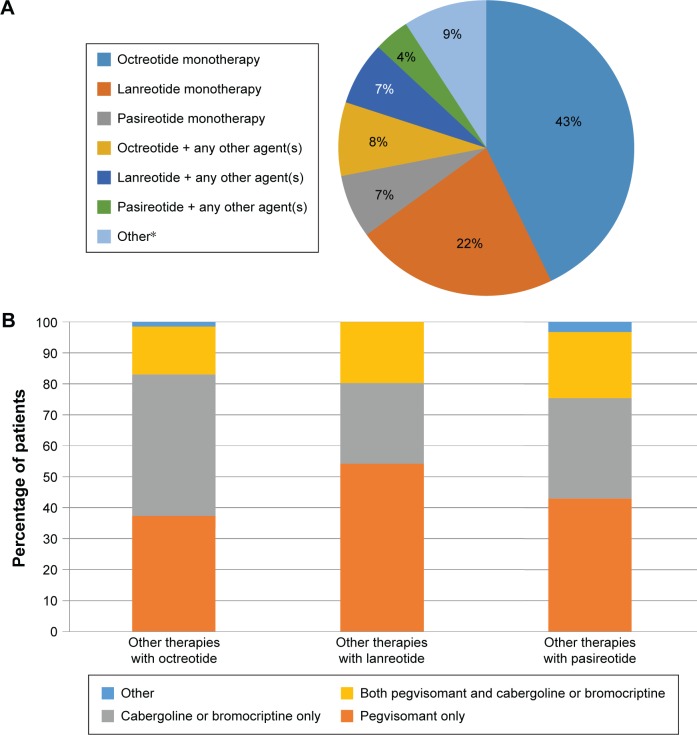
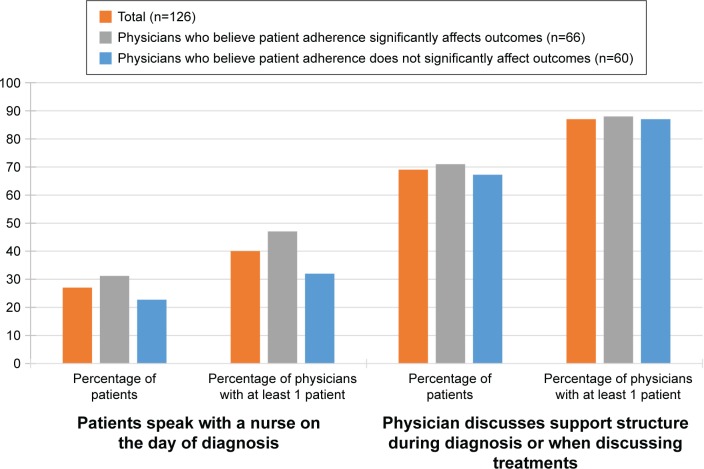
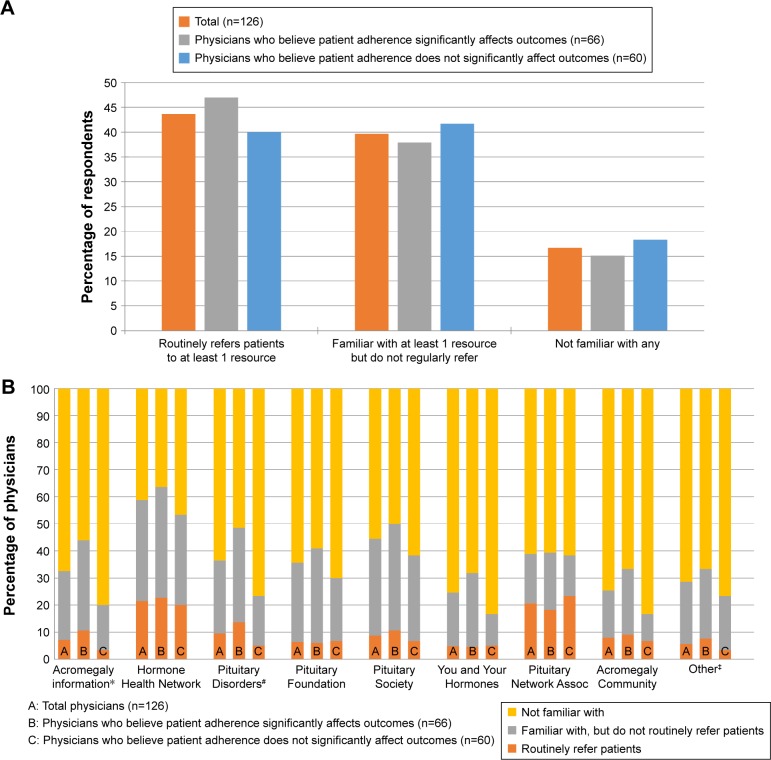
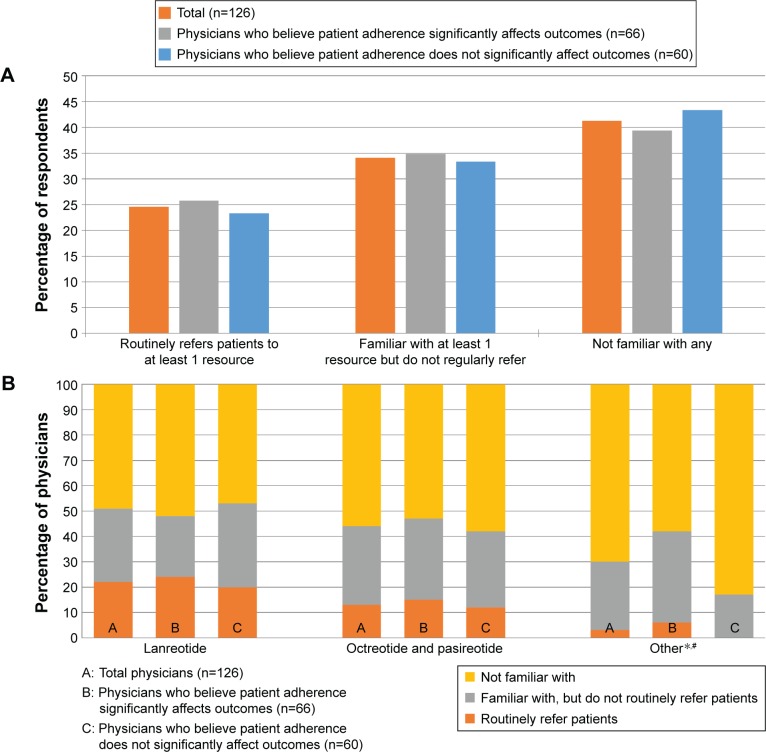
Results: Results are based on responses from 126 physicians from primarily urban and suburban practices, with a median of five acromegaly patients. A total of 70% of patients are currently receiving drug therapy; among these, 91% are on octreotide (51%), lanreotide (29%), or pasireotide (11%), alone or in combination with another therapy. Nearly half of the respondents thought that the impact of patient adherence on therapy outcome for acromegaly was either not very (40%) or not at all (7%) significant. Respondents who believe patient adherence significantly impacts treatment outcome were significantly more likely to discuss automated adherence reminders (50% vs 26%; P=0.015), mobile administration programs (57% vs 35%; P=0.029), and symptom tracking (72% vs 42%; P=0.002). Overall, 44% of respondents routinely recommend education/emotional support programs, and 25% routinely recommend financial assistance programs. Respondents who believe patient adherence significantly impacts treatment outcome generally were more familiar with individual education and emotional support programs compared to those who do not, although they were not more likely to routinely refer patients to any of these resources.
Conclusion: There are unmet needs with respect to increasing awareness among physicians of the importance of patient adherence to therapy, resources available to patients, and how collaboration among patients, nurses, and physicians can improve adherence and overall treatment experiences.
Keywords: emotional support programs; financial support programs; referrals.
Conflict of interest statement
SPB and DG are employees of Deerfield Institute. The authors report no other conflicts of interest in this work.
Figures
Similar articles
-
Pasireotide versus continued treatment with octreotide or lanreotide in patients with inadequately controlled acromegaly (PAOLA): a randomised, phase 3 trial.Lancet Diabetes Endocrinol. 2014 Nov;2(11):875-84. doi: 10.1016/S2213-8587(14)70169-X. Epub 2014 Sep 24. Lancet Diabetes Endocrinol. 2014. PMID: 25260838 Clinical Trial.
-
Treatment adherence and persistence with long-acting somatostatin analog therapy for the treatment of acromegaly: a retrospective analysis.BMC Pharmacol Toxicol. 2017 Apr 4;18(1):22. doi: 10.1186/s40360-017-0124-y. BMC Pharmacol Toxicol. 2017. PMID: 28372573 Free PMC article.
-
The care continuum in acromegaly: how patients, nurses, and physicians can collaborate for successful treatment experiences.Patient Prefer Adherence. 2015 Jul 30;9:1093-9. doi: 10.2147/PPA.S84887. eCollection 2015. Patient Prefer Adherence. 2015. PMID: 26251582 Free PMC article.
-
How to Position Pasireotide LAR Treatment in Acromegaly.J Clin Endocrinol Metab. 2019 Jun 1;104(6):1978-1988. doi: 10.1210/jc.2018-01979. J Clin Endocrinol Metab. 2019. PMID: 30608534 Review.
-
Pasireotide in Acromegaly: A Review.Drugs. 2015 Jun;75(9):1039-48. doi: 10.1007/s40265-015-0413-y. Drugs. 2015. PMID: 26017304 Review.
Cited by
-
Acromegaly and the information gap: patient perceptions of the journey from primary to tertiary care.Endocr Connect. 2020 Oct;9(10):971-977. doi: 10.1530/EC-20-0335. Endocr Connect. 2020. PMID: 33048063 Free PMC article.
-
Treatment Patterns, Adherence, Persistence, and Health Care Resource Utilization in Acromegaly: A Real-World Analysis.J Endocr Soc. 2023 Aug 23;7(10):bvad104. doi: 10.1210/jendso/bvad104. eCollection 2023 Aug 28. J Endocr Soc. 2023. PMID: 37705695 Free PMC article.
-
Observed discordance between outcomes reported by acromegaly patients and their treating endocrinology medical provider.Pituitary. 2020 Apr;23(2):140-148. doi: 10.1007/s11102-019-01013-2. Pituitary. 2020. PMID: 31808101 Free PMC article.
-
Do We Need a Specific Guideline for Assessment and Improvement of Acromegaly Patients Adherence?Front Public Health. 2021 Jul 14;9:693409. doi: 10.3389/fpubh.2021.693409. eCollection 2021. Front Public Health. 2021. PMID: 34336773 Free PMC article.
References
-
- Melmed S. Medical progress: acromegaly. N Engl J Med. 2006;355(24):2558–2573. - PubMed
-
- Rowles SV, Prieto L, Badia X, Shalet SM, Webb SM, Trainer PJ. Quality of life (QOL) in patients with acromegaly is severely impaired: use of a novel measure of QOL: acromegaly quality of life questionnaire. J Clin Endocrinol Metab. 2005;90(6):3337–3341. - PubMed
-
- Colao A, Ferone D, Marzullo P, Lombardi G. Systemic complications of acromegaly: epidemiology, pathogenesis, and management. Endocr Rev. 2004;25(1):102–152. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
